Bone Marrow and Peripheral Stem Cell Transplants
(Hematologic cell transplant HCT)
Patients require a HCT for certain hematologic malignancies such as leukemia, lymphoma, Hodgkin’s disease, and multiple myeloma; myelodysplasia, myelofibrosis and aplastic anemia. Rare conditions such as primary amyloidosis and POEMS syndrome have also benefitted from this therapy. In general there are 2 types of transplants: the autologous where the patient’s own stem cells are re-infused following high dose chemotherapy and allogeneic where another’s stem cells are used. The latter may involve a related donor such as a sibling, an identical twin donor (syngeneic) or an unrelated matched donor. In both cases, the stems cells that are infused will repopulate the bone marrow after high dose myelosuppressive chemotherapy is used to eradicate the malignant hematologic cells. Prior to engraftment, the patient is rendered pancytopenic and totally immunosuppressed making them a high risk for serious infections and hemorrhage. Because of these risks, dental treatment is contraindicated at this time. Patients should be seen prior to the transplant to eradicate dental infection and ensure optimal oral/dental health to prevent dental problems during the period of immunosuppression.
The procedure involves the insertion of a Hickman line (double lumen central venous catheter which is tunneled under the skin to enter the jugular vein), through which chemotherapy and stem cells are delivered. The line usually stays in place until engraftment takes place (approximately 2 weeks with autologous and 4 weeks with allogeneic). If emergency dental care is necessary, the presence of the indwelling catheter necessitates the use of prophylactic antibiotics. The same regimen as the AHA guidelines for cardiac patients is used.

Autologous Peripheral Stem Cell Transplant
The autologous stem cell transplant is a procedure done for certain hematologic malignancies such as multiple myeloma, Hodgkin’s lymphoma, non-Hodgkin’s lymphoma and some types of leukemia. Certain solid tumors such as germ cell tumors may also benefit from this therapy. Higher doses of chemotherapy can be used to eradicate the cancer cells because of the support offered by the stem cells.
The stem cells are collected while the patient is in remission and frozen for later use. The collection process involves mobilization of stem cells. This usually entails infusion of a chemotherapeutic agent such as cyclophosphamide followed by granulocyte colony stimulating factor (G-CSF such as Neupogen® or Filagastrin®). It has been shown that a higher yield of stem cells can be retrieved when the chemotherapy is given initially. Also, the chemotherapy reduces possible tumor cell contamination in the stem cell collection. The cells are frozen and kept stored until the transplant procedure can be performed. After the harvesting but before the transplant, there may be a window of opportunity to perform safe dental care as the blood counts recover shortly after the harvest. It is essential that blood work be reviewed and the presence of a central line be known before any dental work is contemplated. Communication with the oncologist or the nurse coordinator is important.
The next step involves insertion of the Hickman line (if not already in place). Then infusion of the high dose chemotherapy agent is performed. Shortly after, the stem cells are retrieved from the freezer, warmed and infused through the Hickman line. Usually, a period of hospitalization of approximately 2-3 weeks in relative isolation for recovery during which time there will be pancytopenia. More and more, patients are being treated as outpatients and return to the hospital daily for blood work to determine engraftment. Patients may be on prophylactic antibiotics, antifungals and antivirals to prevent opportunistic infections.
Side Effects
The side effects of this therapy are similar to those of any myelosuppressive chemotherapy. As the doses are higher, more severe effects can be seen. Systemic effects such as nausea, vomiting, fatigue, dysgeusia and oral mucositis are not infrequent. Oral effects also include an increase in sensitivity of the teeth especially to cold and dry mouth. Generally, these effects are temporary and empiric treatment such as desensitizing agents and topical anaesthetics are sufficient. However, persistent dry mouth (greater than 3 months) may predispose to the development of root caries and patients should be followed with this in mind. Neutral pH topical sodium fluoride in custom trays may be necessary to prevent severe decay.
Multiple myeloma
Our clinic database reveals that over 2,500 patients with multiple myeloma have been seen. Multiple myeloma is a malignancy of plasma cells. Plasma cells are responsible for producing immunoglobulins and an increase in these proteins are responsible for proteinemia and proteinuria. Also as these cells originate in the bone marrow, symptoms often relate to bone pain, anemia and hypercalcemia. Ten to 15% of multiple myeloma patients have associated amyloidosis. This abnormal protein may be deposited in viscera such as the heart or kidney but does have a propensity to occur in the tongue. When this occurs, the tongue will be enlarged, very hard to palpation and there may be alterations in speech. It can be deposited in other sites in the oral soft tissues as well. Biopsy may be necessary to make a diagnosis. If suspected, it is important to state this as a provisional diagnosis to the pathologist so that special stains for amyloid will be used. (eg Congo Red)
This 67 yr-old male presented with a 6 month history of dysphonia, weight loss and fatigue. Oral examination revealed an enlarged tongue that was very firm to palpation. Note the crenations on the lateral borders with and the increased tissue mass on the right side covering the lingual portions of the crowns of the molars.


Amyloid may significantly affect dental treatment in the following ways:
- If there is cardiac involvement, consultation with the cardiologist may be necessary as prophylactic antibiotics may be recommended
- Renal involvement may decrease renal function and some patients may be on dialysis
- Amyloid in the oral soft tissues may be responsible for the development of hemorrhagic bullae with little trauma
- The physical size and firmness of the tongue may limit the ability to perform routine dental procedures.
As a primary malignancy of bone, multiple myeloma lesions may be present in the jaws. In our experience, approximately 500 patients have lesions in the jaws accounting for 20%. No specific dental treatment is necessary for these but it is important for the dentist to recognize these lesions.
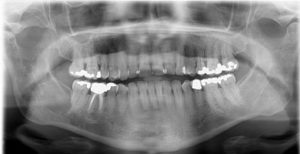
In the following case, the dentist was instrumental in making the diagnosis. This 60 yr-old female presented to her DDS with left TMJ pain with swelling. This pantomograph was exposed and shows a displaced pathologic fracture of the left condyle as well multiple lytic lesions throughout the mandible. The second pantomograph was taken 5 years after the peripheral autologous stem cell transplant with 3 years of intravenous bisphosphonate therapy.




Observations and discussion:
The first image shows a fractured and displaced left condylar head. The bone pattern of the mandible is generally osteoporotic with multiple lytic lesions of varying sizes of the rami bilaterally. The second image taken 5 years later shows the reduced left condylar head but the bone pattern of the mandible appears altered but the prior lytic lesions are barely discernable.
This next example shows a soft tissue mass in the posterior right maxilla of a 54F who had already had a peripheral autologous stem cell transplant for multiple one month previously. She developed this firm soft tissue mass in the right maxillary tuberosity region. It was biopsied and proven to be a myeloma lesion.


The following examples show myeloma involvement of the mandible to varying degrees.











Currently, patients with multiple myeloma are treated with 4 cycles of Cybor-D (Cyclophosphamide, Velcade® {Bortezomib} and Dexamethasone) often accompanied by an intravenous bisphosphonate such as Pamidronate (Aredia®) or Zoledronic acid (Zometa®). Occasionally, Denosumab (Prolia®) is used. This regimen is often followed by an autologous peripheral stem cell transplantation. Maintenance chemotherapy of Lenolidomide (Revlimid®) and intravenous bisphosphonate monthly often follow the transplant pending the response to initial therapy. Please refer to the section on bisphosphonate related osteonecrosis of the jaws (BRONJ or MRONJ) for further details.
Dental treatment plans must take into consideration the presence of the central venous line and blood count values. Prophylactic antibiotics are recommended for the central lines and in patients with absolute neutrophil counts less than 1. The platelet count may also be a mitigating factor. As patients recover, they may be treated as normal. Therefore, it is important to update their medical history keeping these parameters in mind.
Many myeloma patients have involvement of the spine and may have pain when reclined in the dental chair. Also, special head support for cervical spine involvement may be necessary. Consideration of patient comfort and knowledge of the medical condition will promote the patient’s confidence in your care.
Allogenic stem cell transplants
Allogeneic stem cell transplants are indicated for aplastic anemia, leukemias, myelodysplasia, myelofibrosis and lymphoma. Myelofibrosis is a disorder where neoplastic cells stimulate fibrosis and scarring of the bone marrow resulting in pancytopenia. Myelodysplasia (MDS) is a disorder where there is ineffective production of hematopoietic cell lines. Approximately 30% of MDS will progress to acute myeloid leukemia (AML). MDS can be seen after previous chemotherapy for another malignancy. It has also been associated with environmental exposure to certain chemicals such as benzene.
The allogeneic HCT is a procedure that carries significant morbidity and mortality. This type of transplant requires a donor source of stem cells. Related donors especially siblings are preferred; however, only approximately 30% of patients will have a family member match. Therefore, matched unrelated donor (MUD) are done if there is no appropriate family donor. The matching is based on HLA markers. An identical twin donor is referred to as a syngeneic graft. The better the match the better the engraftment with less risk of graft versus host disease (GVHD). For HCT, the patient must be in remission. This is achieved with myelosuppressive chemotherapy regimens based on the disease type. It usually involves induction chemotherapy followed by 2 consolidation or intensification cycles. There may be a window of opportunity to perform dental care safely after consolidation and prior to transplant.
The procedure involves conditioning of high dose chemotherapy and total body irradiation prior to the infusion of the donor cells. This is aimed at removing all of the malignant cells and will render the patient immunosuppressed until engraftment occurs. This requires the insertion of a central venous line (usually a Hickman line) and a period of hospitalization of approximately 4 weeks in isolation for recovery during which time there will be pancytopenia. The chemotherapy places the patient at risk of infection and with the low blood counts, dental care may not safe. Therefore, the patient requires a thorough oral and dental radiographic examination to remove potential sources of odontogenic infection prior to transplantation. Consultation with the hematologist is important to ascertain the patient’s stability for dental treatment. There are no hard and fast rules for this and each patient must be considered on a case-by-case basis. Also, different centres may have differing guidelines as to the use of prophylactic antibiotics. Obvious active dental disease requires treatment and optimal oral health should be attained before hospitalization. The duration of the immunosuppressed period is variable and can be up to one year or more after the transplant. These patients may have the central venous line in situ for this time period and may require frequent transfusions or intravenous drug therapy. For these reasons, safe dental care in the private office setting is variable and thorough review of the medical history is necessary at each visit. A period of isolation, usually averaging at 4 weeks for engraftment follows. Close monitoring for graft versus host disease and other complications will occur for several months to years after the transplant. The patient may be on many medications during this period. These include systemic immunosuppressants (on a tapering dose if no flare of GVHD), antivirals, antifungals, antibiotics, oral bisphosphonates (especially if on long term steroid therapy). Long term steroid therapy will also predispose to diabetes, cataract formation and osteoporosis. The dose of steroid does not require supplemention for dental care.
Factors to consider in the delivery of safe dental treatment include:
- blood counts, particularly platelets and neutrophils
- presence of a Hickman line (requiring prophylactic antibiotics)
- immunosuppressant medications
- presence of graft versus host disease
Oral complications related to bone marrow transplantation include chronic graft versus host disease (GVHD), gingival atrophy, and oral lesions secondary to opportunistic infections. Other lesions described below have been documented in literature and seen in our clinic. The pathogenesis or etiology is unclear.