Post-Radiation Caries
Dental Care After Radiation Treatment
Post-Radiation Caries
The development of caries after therapeutic radiation to the head and neck relates predominantly to the damage to the submandibular salivary glands. As these glands are anatomically located very close to lymph nodes in the neck, they are more often than not, irreversibly damaged. The result is a dry mouth that lacks the buffering capacity of the acidogenic bacteria of the oral cavity. Also, the physical washing of the teeth is decreased causing an increase in plaque formation. Add to this a soft diet which may be high in sugar because of dysphagia and dysgeusia, rampant decay can easily occur and quite rapidly. The mainstay of therapy is prevention with the use of daily topical Fluoride in custom trays and rigorous oral hygiene. Patients must understand that this regimen is a lifelong one. The use of the Modified Schirmer Test (MST) has been a valuable tool in showing our patients that continued hyposalivation exists despite a return to normal eating and tasting long after radiation therapy and that continued use of the Fluoride trays is necessary to prevent caries.
Restoration of post-radiation caries is complex and often compromised. Caries occurs along the cervical margins of the teeth on exposed dentin surfaces.
The significance of post-radiation caries is extremely important. The financial cost of restoring the dentition may be prohibitive; however the risk of osteoradionecrosis with extraction of unrestorable teeth is high and carries significant morbidity.
These initial clinical photos illustrate early erosion with etching of the enamel surfaces. Progression to frank caries is seen if the decalcification continues unchecked without the use of daily fluoride.














Example 1
This 41yr-old male presented with an squamous cell carcinoma of the left oropharynx (HPV +ve) in May 2012 and was treated with concurrent chemotherapy and radiation. He was placed on daily home fluoride in custom trays.




He did not use the fluoride and was referred back to our clinic 2 years later by the surgical oncologist because of “poor dentition”. He has had a number of restorations placed in the interim but continues to have rampant rendering many of his teeth unrestorable. He developed bone exposure spontaneously on the lingual of tooth #37 which subsequently developed into osteoradionecrosis.
Example 2
This 58 yr-old male had nasopharyngeal carcinoma treated with concurrent chemoradiation in Jan, 2012. Fluoride trays were made for him, extraction of 27 and 37 were done and fillings placed in #15,13 and 11




He admitted to not using the Fluoride trays and returned later that year asking that all of his teeth be removed.
Example 3
This 52 yr-old male had a squamous cell carcinoma of the anterior floor of mouth. He was treated with surgical resection followed by radiation.




He did not use the Fluoride trays and continued to smoke. He developed osteoradionecrosis after the teeth in the right mandible were extracted.
Example 4
This 61 yr-old male had a squamous cell carcinoma of the floor of mouth and was treated with surgery followed by radiation.




He did not use the fluoride trays and developed rampant caries necessitating the removal of his remaining teeth. He developed osteoradionecrosis and is slowly healing after hyperbaric oxygen therapy but is still unable to have dentures made because of exposed bone.
Example 5
This 64 yr-old male was treated with radiation therapy for a carcinoma of the nasal fossa.




He did not use the fluoride trays and developed rampant decay necessitating removal of the remaining teeth.
The Dilemma of Post-radiation Caries
The above examples are extreme ones and pose severe challenges to the dentist. In the non-radiation setting, a solution of total dental extraction with denture fabrication would be the treatment of choice. However, given the risk of osteoradionecrosis with extractions post-radiation, this option must be considered carefully. These are the principles that are used to minimize this catastrophic problem:
- Patient Education Prior to Radiation TherapyAt the initial consultation, the potential side effects are thoroughly explained to the patient and accompanying family members. Clinical photographs illustrating post-radiation caries and osteoradionecrosis are displayed in each operatory to reinforce this message and the importance of daily home fluoride therapy are stressed.
- Case Selection for Extraction Prior to Radiation TherapyThis may be the most challenging clinical decision that the dentist must make. The decision whether the teeth will be sustainable for the life of the patient depends on many factors. The usual sound dental criteria used for extraction – abscessed teeth, unrestorable caries and severe periodontal disease make this decision easier; however, the patient’s dental IQ, oral hygiene, motivation to preserve the dentition and compliance with stricter oral hygiene with fluoride are factors that may be more difficult to assess. For example, patients who continue to smoke after the diagnosis of oral cancer may not be as compliant or motivated to do what is necessary to maintain their dentition after treatment.
- Close Follow-Up During and After Radiation TherapyPatients are seen half way through their radiation treatment to address oral care. Acute mucositis may preclude the use of the fluoride trays or even routine oral hygiene procedures. The use of topical anesthetics (mucositis rinse) before F use may be beneficial. Discontinuation of the use of toothpastes with sodium lauroyl zsulfate for brushing may also help when mucositis prevents brushing. The use of sodium bicarbonate on a wet toothbrush may be used instead of dentifrices.
Patients are seen one month after the radiation therapy has been completed. At this time, the MST is measured and F tray use is reinforced and emphasized. If patients are still eating only soft foods, liquids or feeding tube dependent, fastidious oral hygiene is even more important as these foods stick to the teeth in a dry mouth and promote dental decay. Early detection of post-radiation caries when restoration is possible is paramount in maintaining the dentition. It is our experience, amalgam restorations are superior over composite resins in a dry mouth. Full coverage crowns are discouraged until the establishment of a caries-free stable period. The use of bonded amalgam for extensive class V caries that wrap around the cervical margins of the teeth are the treatment of choice in our clinic.
Dental radiographs especially bitewings and periapical views of the anterior teeth are necessary to detect interproximal root caries that may not be clinically apparent. There is NO contraindication to dental radiography after treatment.



In this example, the clinical appearance of these non-mobile, asymptomatic lower incisors might indicate that these teeth are restorable. The periapical image however, indicates that they are not.


- When Teeth Are UnrestorableThere are many factors that require consideration for dental extraction and care must be made to minimize this risk. Balancing these factors to determine the risk vs. benefit ratio of the procedure requires that the patient understands the serious implications and makes an informed decision. There are no strict guidelines as each patient’s circumstances are unique. It may seem unthinkable to the conscientious dental practitioner to leave decayed teeth in place and untreated; however, if there are no symptoms and there is substantial risk of osteoradionecrosis, it may be in the patient’s best interests to observe and treat when there are symptoms of pain or infection.
- SymptomsOften post-radiation caries are totally asymptomatic. The presenting features may be aesthetic concerns or rough, sharp edges of carious lesions irritating the adjacent soft tissues. Toothache pain per se is relatively rare given the extent of the carious lesion. The option of prophylactic or prescribed endodontic therapy with amputation of the remaining crown may be considered for the isolated tooth.
- Compliance with F Care, Oral Hygiene and Dental IQIf the patient has not been compliant with the F trays and there is generalized post radiation caries, some of which may be restorable with extensive endodontic therapy and complex restorations, it may be prudent to have a frank discussion with him/her about the goals of therapy. If after spending significant sums of money to restore the dentition the patient may be very disappointed to have it fail because of lack of compliance. Selective extractions and restorative work to regain function may be an option. Extensive crown and bridge work is not recommended until the patient has had at least a one year free of caries and compliance with F therapy is well-established.



Extractions After Radiation Therapy
There are several parameters requiring consideration for post-radiation extraction. Weighing these factors will give some indication of the level of risk of osteoradionecrosis. There are no hard and fast rules, but the following guidelines may aid in this deliberation.
- Site – is the tooth in question in the mandible or maxilla?
- Osteoradionecrosis is more common in the mandible partly because the microcirculation mandible is different from the maxilla. i.e given the same radiation dose, the risk of ORN is less in the maxilla than the mandible.
- Is he tooth in the field of the prior radiation?
- The dose of radiation is important to know as the risk increases over 50Gy. This information may only be available to receive from the radiation oncologist. Patient consent to contact this physician will be necessary.
- Symptoms – is the patient experiencing pain or swelling?
- Acute symptoms may need to be treated with antibiotics and analgesics until all of the required information is obtained.
- Patient factors
- Smoking & Comorbidities
- Patients who continue to smoke after radiation therapy will have an increased risk of osteoradionecrosis if teeth require extraction. Smoking cessation programs are encouraged.
The following examples are illustrative of a common sequela of radiation therapy to the jaws. Increased widening of the periodontal ligament space and increased sclerosis are indicative of radiation damage to the bone. It is essential that the dentist recognize that these changes may NOT represent dental inflammatory disease. Given the history of prior radiation therapy, the dentist must do a thorough clinical examination including pulp testing if they are concerned for infection of odontogenic origin. If teeth are asymptomatic and vital, dental intervention is not indicated as extractions and unnecessary root canal therapy may precipitate osteoradionecrosis.
Case 1
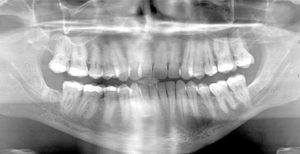
This 51 yr-old male had radiation therapy for laryngeal carcinoma. This pre-treatment panorex shows a fairly intact dentition. F trays were made for him as no other dental care was necessary.


This post-radiation panorex was taken 2 ½ years later and shows obvious post-radiation caries and of note, widening of the periodontal ligament space around tooth #47. It was not sensitive to percussion or mobile.


Case 2
This 45 yr-old female was treated with post-op radiation therapy for a squamous cell carcinoma of the right side of the tongue in 2012. The cropped panoramic image on the left was exposed at that time. The cropped panoramic image on the right was taken in 2015. There is widening of the periodontal ligament spaces of teeth # 45, 46 and 47. These teeth are not sensitive to percussion or mobile and she has been diligent with oral hygiene and F care.




Case 3
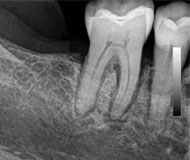
This 50 year-old male received concurrent chemotherapy with IMRT radiation therapy in August, 2012 for a squamous cell carcinoma of the right tonsil. Prior to his treatment tooth #28 was extracted and F trays were made. The following periapical film was taken in Jan, 2015 when he presented with pain associated with tooth #48. It was mobile and sensitive to percussion but non-carious. Note the widening of the periodontal ligament space of both teeth # 47 and #48 with surrounding sclerosis.


Unlike the previous cases, the clinical symptoms here indicated infection of the 48.


Case 4
This 65 year-old female was treated for a squamous cell carcinoma of the left mandibular alveolus with surgical resection followed by radiation therapy in 2012. Her family dentist referred her back because of the radiographic changes seen in the periapical taken November, 2013. She was totally asymptomatic. The teeth in the fourth quadrant were all slightly mobile but not sensitive to percussion. Note the uneven widening of the periodontal ligament space of the mesial and distal roots of teeth #45 and #46. There is an increase in sclerosis as well. There is evidence of progression of periodontal bone loss as well.



Case 5
This 49 year-old male was treated with radiation and concurrent chemotherapy for a HPV +ve squamous cell carcinoma of the left tonsil in Oct, 2010 when the first pantomograph was exposed. The second one was taken in December of 2013. He was completely asymptomatic and the teeth were not mobile. Note the widening of the periodontal ligament spaces of the posterior mandibular teeth.



Case 6
This 54 yr-old female was treated with radiation and concurrent chemotherapy for nasopharyngeal carcinoma in July 2009 when this first pantomograph was taken. The second was exposed in September, 2013. There is obvious widening of the periodontal ligament spaces of the mandibular teeth with increased sclerosis. The third one was taken in July 2015 shortly before tooth #44 spontaneously exfoliated. There was no pain but the teeth were mobile.






Case 7
In this example, the patient is a 59F who was treated with chemoradiation in 2004 for base of tongue squamous cell carcinoma. The image on the left (cropped pan) was taken in 2009 and shows widened periodontal ligament space of teeth #35,36, and 37. These teeth were totally asymptomatic and a decision to observe them was made. The image on the right was taken in 2014 and the prior changes are only very slightly detectable.




Case 8
This 60 yr-old male was treated for a T2N2M0 squamous cell carcinoma of the left oropharynx in June of 2012. The image on the left is from a cropped panoramic image taken at that time. The image on the right is a periapical film exposed in December of 2015. This image is slightly foreshortened but shows a diffuse area of radiolucency between the roots of #46 and #47 extending to the furcation areas of both molars. They are not mobile, sensitive to percussion and test vital with cold testing.




Removing teeth that were in the field of high dose radiation carries a substantial risk of the development of osteoradionecrosis. Care must be made that extraction is absolutely necessary and that the patient is aware of the potential sequela. The radiographic appearance of widened periodontal ligament space (PDL) mimicking rarefying osteitis is NOT necessarily an indication for extraction. Widened periodontal ligament space with adjacent sclerosis under normal conditions connotes an inflammatory process. However, after therapeutic doses of radiation therapy, this change may be related more to the radiation damage to the bone and not be odontogenic in etiology. Accurate diagnosis is paramount.
We have determined with a recent research project that widened PDL is the most common change detected in panoramic images after radiation therapy accounting for 88% of the changes observed. This is extremely important to recognize to obviate the need for extraction with its attendant risk of osteoradionecrosis.
Chan, KC, Perschbacher, SE, et al: Mandibular changes on Panoramic imaging after head and neck radiotherapy. Oral Surg Oral Med Oral Pathol Oral Radiol 2016; 121:666-672 This paper from our institution has been recognized by the Journal of the American Dental Association as the fist large case series to document and characterize subclinical mandibular changes. It has also been awarded the best research paper in the radiology section of this journal for 2015/16.
Guidelines for Post-XRT extractions
Please note that these are general guidelines and not hard and fast rules. There will be exceptions and each patient’s medical history and radiation details must be taken into account as mitigating factors as well as the dental status and nature of the presenting signs and symptoms. In some circumstances, if the clinical judgment of the dentist is that the risk outweighs the benefits of extraction, the unrestorable tooth may be left in place and treated by root canal if symptomatic. There is no evidence or data to support the following statements and they are based only on our experience.
- Site
- It is always prudent to consult with the patient’s radiation oncologist to find out the dose to the tooth and surrounding bone that requires extraction. Patients may not remember the precise area of treatment and there may be hot spots not related to the site of the tumour that would have received significant dose. If the dose was less than 50 Gy, simple extraction would result in a low risk of delayed healing.
- Osteoradionecrosis (ORN) is generally rarer in the maxilla. This may be due to the vascular supply of the maxilla being different from the mandible and the fact that the mandible is more likely to be in the field of treatment because tumors and lymph nodes more commonly affect these sites. However, for maxillary sinus, palatal salivary gland and nasopharyngeal carcinomas, the dose to the maxilla may be significant and increase the risk of ORN.
- Surgical Difficulty of Extraction
- Any extraction requiring reflection of a full thickness mucoperiosteal flap procedure, carries a greater risk of delayed healing and possible osteoradionecrosis. This is especially true in the posterior mandible where the periosteum is a major source of vascular supply to the mandible after radiation therapy. Therefore avoidance of raising a flap is an important surgical principle. Removal of adjacent bone circumferentially around the tooth root may be an alternative
- Medical Co-Morbidities
- Patients who continue to smoke tobacco, have peripheral vascular disease, diabetes or who are taking oral bisphosphonates for osteoporosis are also at greater risk of delayed healing and possible osteoradionecrosis. Elderly, frail patients may also have delayed wound healing.
- If the patient has metastatic disease or a poor prognosis, palliative or no treatment should be considered.
- Surgical Techniques
- The role of prophylactic hyperbaric oxygen is controversial and may not be available for a dental emergency.
- The use of prophylactic antibiotics is also unproven in oral extraction site healing.
- If many teeth need to be removed, it is prudent to start with a few teeth not in the field of treatment in different quadrants, so as to leave a smaller wound. If these areas heal satisfactorily, further extractions can be carried out. If they do not heal, further extractions should be avoided.
- After the tooth is removed, interradicular/interseptal bone and any other sharp pieces should be removed or smoothed off to prevent sequestration.
- Primary closure with sutures and packing with either absorbable gelfoam or collagen plugs to obtund the socket to prevent food and debris from filling the defect is also recommended.
- Follow-up at least one week post-extraction to assess the wound healing is important. At this time, the patient may be shown how to irrigate the socket with a monoject syringe to keep it clean if necessary.
Summary
Patient education is paramount to prevent the need for extractions in the post-radiation setting. All invasive surgical procedures including but not limited to implant placement, periodontal and endodontic surgery should be considered contraindicated in the site of high dose radiation therapy. Close follow-up with emphasis on topical fluoride treatment, abstinence from sugary food and drink, meticulous oral hygiene and restoration of early root decay are necessary to maintain a healthy dentition.