Head & Neck Cancer
Head & Neck Cancer Patients
Diagnosis & Treatment
In North America, cancer of the head and neck comprises from 3-5% of all cancer. Generally, these cancerous growths occur from the base of the skull to the thyroid gland and include the nasal cavity and paranasal sinuses, nasopharynx, oral cavity, oropharynx, hypopharynx, supra and subglottic larynx, cervical oesophagus, skin, salivary glands and metastasis to the neck from unknown primary sources. The vast majority (>75%) are squamous cell carcinomas with salivary gland, lymphoma and sarcomas occurring in order of decreasing frequency. The anatomic proximity to the oral cavity, teeth and jaws underscore the important roles of the dental health care professional.
The Dentists Role
The dentist is often the first health care professional consulted by a patient with signs and symptoms of cancer of the head and neck. Swelling and pain are often symptoms accompanying dental pathology and a careful history, examination and radiographic evaluation must be performed to rule out odontogenic sources of these symptoms. Even when there are no symptoms, the ability of the dentist to detect mucosal abnormalities in the early stages is superior to other health care providers simply due to clinical experience. Non healing ulcers, red lesions, red and white lesions, white lesions and irregular masses require either further investigation or close follow-up to ensure that appropriate treatment is done. A level of suspicion should be followed up on any oral lesion that does not heal and is not yet diagnosed as some other mucosal abnormality. Risk factors for oral cancer include: advancing age (>60yrs); combined use of alcohol and tobacco, other tobacco use (such as smokeless tobacco, snuff, betel nut) and being immunocompromised. Biopsy or referral for biopsy by the dentist can reduce the delay in diagnosis significantly. Referral to an oral surgeon for biopsy may lead to an earlier diagnosis than referring the patient to his/her family physician. Early diagnosis is still the most important factor in improving overall prognosis of malignant disease of the head and neck region.
The following 3 photographs illustrate early squamous cell carcinomas presenting as irregular raised red and white areas on the lateral tongue; posterior lateral tongue extending to the floor of mouth and buccal mucosa. All of these would be readily visible in a dental oral examination.





The Role of Dental Imaging
The dentist is also in the unique position to be able to radiograph the jaws. Suspicious intrabony lesions may mimic the common inflammatory conditions of periodontal and periapical disease. Careful attention to the clinical history, examination findings combined with unusual radiographic features should raise the level of suspicion that warrants further investigation or at least referral to an oral and maxillofacial radiologist.
Intraoral films, periapical and occlusal projections provide the best resolution and can detect early and subtle changes that may occur from intrabony malignancies.
This example of malignant lymphoma as seen in 3 intraoral periapical films of the mandibular anterior region shows irregular bone destruction with loss of the lamina dura along the distal root of 31 and mesial and distal root surfaces of #32 and apical regions of 33 and 34. The bone pattern in these areas show an infiltrative process that is not well delineated. Periodontal bone loss would occur from the coronal portion apically and periapical rarefying osteitis would be centred around the apex or apices of the involved teeth.


Occlusal views provide benefits such as visualizing the entire lesion as well as the perspective of a view at right angles to the periapical or panoramic view. The integrity of the lingual cortex and expansion give valuable clues as to the nature of the lesion.


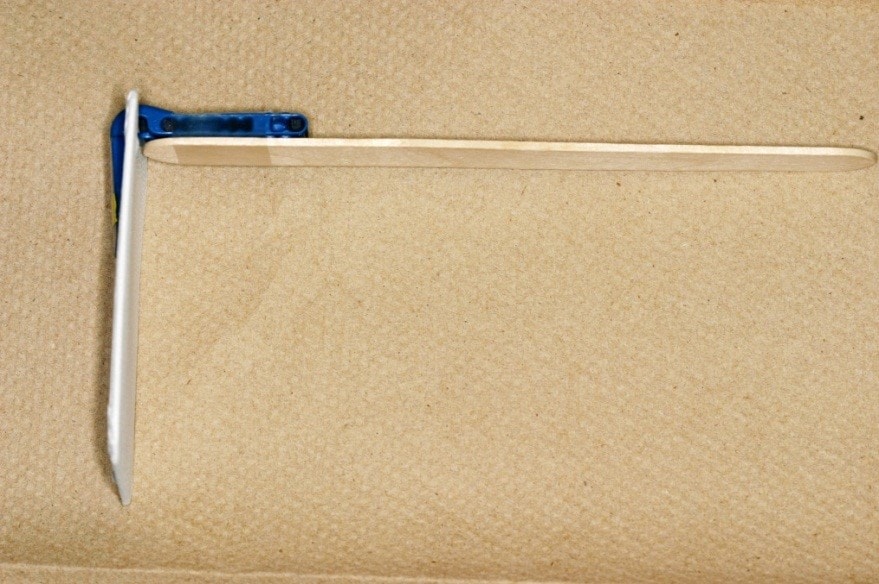
This occlusal film is an extraoral tangential projection to show a sagittal view of the anterior mandible. In this example, an ill-defined radiolucent entity has destroyed the labial cortex of the anterior mandible. The technique used to produce this image is shown.


The occlusal film is taped to a stabe film holder and a tongue depressor. The patient is then asked to bite on the tongue depressor so that the film is centred over the region of interest. The beam is lined up to reach the film at 90 degrees.



Panoramic radiographs provide an overall view of the maxilla, mandible and are useful to compare the right and left sides. In this example of a left maxillary sinus carcinoma, the cortical boundaries of the posterior border of the maxilla, the posterior border of the maxillary sinus and the floor of the sinus are easily seen on the right side (arrows) but are absent on the left side where the malignancy has destroyed these landmarks.


In this case, the changes are more subtle. The floor of the left maxillary sinus is partially destroyed and an irregular soft tissue mass can be seen.


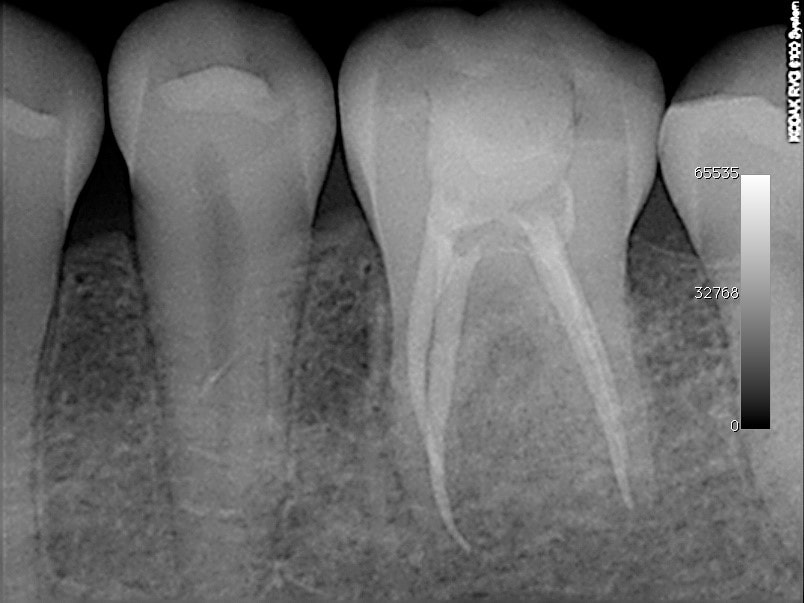
In this example, a young patient presented with pain and swelling. The dentist performed root canal therapy on #36 without resolution of the symptoms. Clinically, a bony hard swelling was seen on the buccal attached gingiva. The periapical film shows the interradicular bone to be abnormally sclerotic in pattern with loss of definition of the root surfaces. There is slight widening of the mesial periodontal ligament space. This is an example of osteosarcoma. It would not be expected that the dentist who initially saw this patient would be able to make this diagnosis; however, the clinical presentation of a bony hard swelling (not usual in dental infection), lack of caries or source of periapical inflammation and the unusual radiographic appearance should have at least raised a level of suspicion that the film be reviewed by an oral and maxillofacial radiologist who would be able to make this interpretation or have it in a differential diagnosis.



In general, the radiographic signs of malignancy include: irregular bone destruction with an ill-defined border and lack of cortication; patchy destruction with an infiltrative pattern, widening of the periodontal ligament space with destruction of the lamina dura, loss of cortical boundaries such as the sinus floor, interior border of the mandible; the appearance of tooth floating in space.
Head and Neck Cancer Patients
The type of cancer of the head and neck region at our institution is approximately comprised of squamous cell carcinoma 75%; salivary gland malignancy 8% and nasopharyngeal carcinoma 11%, with the remaining 6% represented by rarer entities including lymphoma and sarcoma.
As of June 30, 2015 the Head and neck cancer patients seen in our clinic by site was 12,727 with the following breakdown:
| Site | Total # | % |
|---|---|---|
| Oral cavity (including floor of mouth, tongue) | 2,820 | 22% |
| Oropharynx (including tonsil, base of tongue) | 2,410 | ~19% |
| Glottic (including larynx, supraglottic,hypopharyngeal) | 2,696 | 21% |
| Nasopharynx | 1346 | 11% |
| Salivary gland | 1030 | 8% |
| Maxillary/paranasal sinuses | 488 | 3.8% |
| Unknown primary with neck | 743 | 5.8% |
| Nose/nasal fossa | 160 | 1.2% |
| Miscellaneous – skin, sarcoma, esthesioneuroblastoma, ear canal carotid body tumors | 1034 | 8% |
The Role of Human Papilloma Virus (HPV) in Head and Neck Cancer
The incidence of head and neck squamous cell carcinomas has shown a slow, steady increase over the past few decades. In the past, the type of patients affected were more commonly those who smoked cigarettes and drank alcohol in excess. With successful smoking cessation programs leading to an overall decrease in the percentage of people smoking, the increase in incidence of head and neck cancer support other etiologic factors. It is now well-established that HPV plays a role in the etiology of oropharyngeal, base of tongue and tonsillar squamous cell carcinoma. The HPV positive type of squamous carcinoma represents a specific clinicopathologic entity in that it occurs in patients without the known risk factors of smoking and alcohol use and histologically has a characteristic “basaloid” appearance to the epithelial cells. This has been well documented in oropharyngeal carcinomas only. The role of HPV in other head and neck sites has not been clearly established. The source of HPV infection has been determined to be sexual transmission (oral-genital contact). HPV infection as a sexually transmitted disease is very common; however, the factors associated with ability for incorporation of the HPV DNA to cause oropharyngeal cancer is unknown. It may take many years for this to occur. Currently the number of oropharyngeal cancers related to HPV approximates 70-80% or 13% of our head and neck cancer patients. It is more common in males and is suspected when other risk factors such as smoking and alcohol use are not relevant. There is much ongoing research into the determinants leading to cancer from infection. An important feature is that the response to current treatment regimens with improved survival rates and risk of progression for an HPV-related oropharyngeal carcinoma is significantly better than a non-HPV related ones. With the advent of effective vaccines against HPV, the rates of infection and later oropharyngeal cancer may be significantly reduced as is expected with cervical cancer. In summary, HPV related oropharyngeal carcinomas:
- Occurs more commonly in males (4.5:1), with an average age of 58 yrs
- Without other known risk factors (smoking and alcohol)
- May present as a metastatic lymph node in the neck
- Have a characteristic histologic appearance (basaloid or reticular epithelium)
- Have a better prognosis than non HPV-related oropharyngeal carcinomas
Nasopharyngeal Carcinoma
Nasopharyngeal carcinoma (NPC) is also a distinct clinicopathologic entity that has significant distinctive features that warrant a separate discussion. The name is not only indicative of the specific site of occurrence but connotes several distinguishing features. At this site, 2 types of squamous carcinomas occur – the first is a non-keratinizing type and the second is a keratinizing type. The non-keratinizing form (NK) is etiologically related to the Epstein Barr virus (EBV) and is seen with unique demographics. A geographic predisposition of southeast Asia, the Arctic, Middle East and North and South Africa. The most common presenting symptom is a nodal swelling in the neck. In this type, circulating antibodies to EBV are found and titres may be used to monitor the presence of disease. Epistaxis or nasal obstruction may also be presenting symptoms. This particular type of cancer is radiosensitive.
Head and Neck Cancer Treatment
Therapy for head and neck cancer consists of any or all of the usual modalities of cancer treatment including radiation therapy, surgery and chemotherapy. The type of therapy is dependent of the precise anatomic location, stage of the disease, type of malignancy and patient factors such as comorbidities. The protocols are always evolving as results of clinical trials are incorporated into the standards of care. Multidisciplinary tumor boards are effective in the discussion of the best treatment protocol taking all of these factors into consideration to provide individualized or patient-centred therapy. The treatment relies heavily on the stage of the disease. For details on how the stage of disease is determined, please refer to this link.
For details of specific treatment regimens for head and neck cancer, please refer to the Clinical Practice Guidelines of the Head & Neck Site group of Princess Margaret Cancer Centre.
In general, the following site specific guidelines are considered:
-
-
Laryngeal Cancer
For squamous cell carcinomas of the larynx, the general management approach is laryngeal/pharyngeal function preservation using a radical radiotherapy approach with or without chemotherapy and neck dissection for disease in the neck as required reserving total laryngectomy or hemilaryngectomy for radiation failures. Surgical resection with post-operative radiotherapy or chemoradiotherapy is reserved for gross extralaryngeal extension or when the likelihood of a functional larynx or pharynx after primary radiotherapy or chemoradiotherapy is minimal.
- a. Early or localized disease Stage I-II
Patients with early glottic cancer may be treated either by external beam radiation therapy or conservation surgery such as endosopic laser excision or partial laryngectomy.
Patients with early supraglottic cancer may be treated with either external beam radiation therapy or conservation surgery. Radiotherapy for this group usually includes prophylactic bilateral treatment of level II-III lymph nodes in the neck. Endoscopic laser excision or supragottic laryngectomy with selective neck dissection to include levels II-III nodes may be considered for patients with early supraglottic cancer. Bilateral neck dissection should be considered if the tumor is close to the midline. - b. Locally Advanced Laryngeal Cancer Stage III-IV
Patients with locally advanced resectable laryngeal cancer can be treated by either total laryngectomy with or without post-operative radiation therapy or initial organ preservation strategy with radiation and concurrent chemotherapy, reserving surgery for salvage.
- a. Early or localized disease Stage I-II
-
Hypopharyngeal Cancer
For squamous cell carcinomas of the hypopharynx, laryngeal/pharyngeal function preservation using a radical radiotherapy approach with or without surgery for the neck as required.
- a. Early Stage I-II
Patients with early hypopharyngeal cancer may be treated with radical external beam radiation therapy with concomitant chemotherapy and prophylactic irradiation of neck nodes or conservative surgery and selective bilateral neck dissection; or radiotherapy alone including altered fractionation regimes in those patients who are not suitable for either concurrent chemotherapy or surgery due to comorbidities. - b. Stage III-IV
Patients with locally advanced resectable hypophyaryngeal cancer can be treated by either surgical resection with postoperative radiation therapy or radiation with concurrent chemotherapy or altered fractionation radiation reserving surgery for salvage as an organ presevation strategy.
- a. Early Stage I-II
-
Oropharyngeal cancer
Management of early oropharyngeal squamous cell cancer should be individualized for each patient. Decisions regarding the choice of primary treatment modality should be made in consultation with the patient and should take into account the anatomic location of the tumor and the functional results associated with the available treatments. Oropharyngeal function/organ preservation using a radical radiotherapy approach with or without surgery for the neck as required is the usual approach undertaken. Oropharyngeal primaries always require elective treatment of regional lymph node regions at risk of involvement.
- a. Stage I-II
Patients with early oropharyngeal cancer may be treated by primary resection or external beam radiation therapy encompassing the primary tumor and neck nodes. - b. Stage III-IV
For organ preservation therapy, radiation therapy with concurrent cisplatin chemotherapy with neck dissection if there is clinical or radiologic evidence of residual disease.
- a. Stage I-II
-
Oral Cavity Cancer
Management of oral cavity (buccal mucosa, oral tongue, floor of mouth, lip, retromolar trigone, hard palate mucosa, alveolus) squamous cell cancer should be individualized for each patient. Decisions regarding the choice of primary treatment modality should be made in consultation with the patient and should take into account the anatomic location of the tumor and the functional results associated with the available treatments. Organ and function preservation using surgery with or without reconstruction and neck dissection if required and post-operative radiotherapy with or without chemotherapy is the standard approach. Radical radiotherapy with or without chemotherapy is considered when surgical morbidity at the primary site is anticipated and considered inappropriate; if the patient declines surgery, has unresectable neck disease and primary not yet surgically treated. Post-operative radiotherapy should be idealy started within 6 weeks of surgery.
- a. Stage I-II
Patients with early oral cavity cancer may be treated by surgical resection taking into account the anatomic location and functional results possible. Post-operative radiation therapy should be considered for patients with clinical and pathologic features that indicate a high risk of recurrence. - Stage III-IV
If the tumor is resectable, surgery with post-op radiation or primary radiation therapy with concurrent chemotherapy may be considered.
- a. Stage I-II
-
Nasopharyngeal carcinoma
As these tumours are considered to be radiosensitive, radiation with concurrent chemotherapy is usually the treatment of choice. For stage 1 disease, radical radiotherapy is the standard. For stages II-IV, primary radiotherapy with concurrent with or without adjuvant chemotherapy is the standard care.
-
Salivary gland malignancy
Generally primary surgical resection is the preferred treatment with post-op radiation therapy for positive or close margins, extracapsular extension of nodal disease and perineural or lymphovascular involvement. Chemotherapy is not generally indicated for salivary tumors. Rarely, radiotherapy is used as a sole modality where disease is unresectable or if surgery cannot be done for other reasons.
-
Paranasal sinuses
Management of squamous cell carcinoma of the paranasal sinuses should be individualized for each patient. Decisions regarding the choice of primary treatment modality should be made in consultation with the patient and should take into account the anatomic location of the tumor and the functional results associated with the available treatments. Treatment decisions should involve the patient and take into account their preference once informed of their options. Treatment options include:
- Pre-operative moderate dose radiation therapy followed by definitive surgical resection
- Definitive high dose radiation therapy with or without concurrent chemotherapy with surgery reserved for salvage
- Primary or definitive surgical resection followed by post-operative radiation therapy with or without concurrent chemotherapy.
-
Unknown primary with neck metastases
-
When a lymph node in the neck contains metastatic deposits of squamous cell carcinoma, the most common primary site is the oropharynx. i.e. base of tongue or tonsil. In the south east Asian demographic, nasopharyngeal carcinoma may be considered. However, on occasion, the primary site cannot detected. Radiation therapy with or without chemotherapy with post-operative surgical neck dissection depending on the stage and nodal involvement is considered. As always, management is individualized for each patient and advice from a multidisciplinary tumour board should be taken into account.
Radiation Therapy
Radiation therapy (sometimes abbreviated to XRT) is the medical use of ionizing radiation as part of cancer treatment to control malignant cells (not to be confused with radiology, the use of radiation in medical imaging and diagnosis). Radiotherapy may be used for curative or adjuvant (enhancing the action of a medical treatment) cancer treatment. Radiotherapy is used for the treatment of malignant tumors (cancer), and may be used as the primary therapy. It is also common to combine radiotherapy with surgery, chemotherapy, or a combination of the three. Most common cancer types may be treated with radiotherapy in some way. The precise treatment intent (curative, adjuvant, neoadjuvant, therapeutic, or palliative) will depend on tumour type, location, and stage, as well as the general health of the patient.
Radiation therapy is commonly applied to the cancerous tumour. The radiation fields (the amount of tissue to be treated ) may also include the draining lymph nodes if they are clinically or radiologically involved with tumour, or if there is thought to be a risk of subclinical malignant spread. It is necessary to include a margin of normal tissue around the tumour to allow for uncertainties in daily set-up and internal tumor motion. These uncertainties can be caused by internal movement (for example, breathing).
To try to spare normal tissues (such as skin, saliva glands or organs which radiation must pass through in order to treat the tumour), shaped radiation beams are aimed from several angles of exposure to intersect at the tumour, providing a much larger absorbed dose there than in the surrounding, healthy tissue.
Radiation therapy works by damaging DNA of cancer cells.
The amount of radiation used in radiation therapy is measured in gray (Gy), and varies depending on the type and stage of cancer being treated. For curative cases, the typical dose for a solid epithelial tumor (most head and neck cancers) ranges from 60 to 80 Gy, while lymphoma tumors are treated with 20 to 40 Gy.
The total dose is fractionated (spread out over time) for several important reasons. Fractionation allows normal cells time to recover, while tumor cells are generally less efficient in repair between fractions. In North America, Australia, and Europe, the typical fractionation schedule for adults is 1.8 to 2 Gy per day, five days a week.
In some cases, two fractions per day are used near the end of a course of treatment. This schedule, known as a concomitant boost regimen or hyperfractionation, is used on tumors that regenerate more quickly when they are smaller. In particular, tumors in the head-and-neck demonstrate this behavior.
Before treatment, a CT scan is often performed to identify the tumor and surrounding normal structures. The patient is then sent for a simulation so that moulds (an immobilization mask) can be created to be used during treatment.




Radiation is delivered in many different ways; two that are highlighted are conventional external beam radiotherapy and Intensity Modulated Radiation Therapy.
Conventional external beam radiotherapy (2DXRT) is delivered via two-dimensional beams using linear accelerator machines. 2DXRT mainly consists of a single beam of radiation delivered to the patient from several directions: often front or back, and both sides.
Intensity-Modulated Radiation Therapy (IMRT) is an advanced type of high-precision radiation. Computer-controlled x-ray accelerators distribute precise radiation doses to malignant tumors or specific areas within the tumor. The radiation dose is consistent with the 3-D shape of the tumor by controlling, or modulating, the radiation beam’s intensity. The radiation dose intensity is elevated near the gross tumor volume while radiation among the neighboring normal tissue is decreased or avoided completely. The customized radiation dose is intended to maximize tumor dose while simultaneously protecting the surrounding normal tissue. This may result in better tumor targeting, lessened side effects, and improved treatment outcomes.
Radiation therapy is in itself painless. Treatment to higher doses causes varying side effects during treatment (acute side effects), or in the months or years following treatment (long-term side effects). The nature, severity, and longevity of side effects depends on the organs that receive the radiation, the treatment itself (type of radiation, dose, fractionation, concurrent chemotherapy), and the patient.
Most side effects are predictable and expected. Side effects from radiation are usually limited to the area of the patient’s body that is under treatment. One of the aims of modern radiotherapy is to reduce side effects to a minimum, and to help the patient understand and deal with those side effects which are unavoidable.
As the epithelium of the oral cavity is turning over rapidly, it is also targeted inadvertently by the radiation resulting in breakdown. Mucositis begins 1-2 weeks into the radiation Confluent ulceration with erythematous borders in a background of generalized “whitening” of the oral mucosa is often seen. This is the major source of pain, dysphagia, weight loss and overall debilitation during radiation therapy. If severe, this can affect swallowing, and the patient may need analgesics and nutritional support/food supplements. A feeding tube may be placed temporarily if the patient has difficulty swallowing. Treatment is empiric and consists of systemic analgesics, topical anaesthetics (mucositis rinse) and change is diet to soft, bland foods.
The Role of Chemotherapy in Head and Neck Cancer
Chemotherapy in combination with surgery or radiation as first-line treatment of head and neck cancer is used in patients with locally adanced non-metastatic squamous cell carcinoma of the oral cavity, oropharynx, larynx and hypopharynx who are medically fit for chemotherapy. Concurrent chemotherapy is considered over radiation alone if organ preservation is the goal and the primary tumour is unresectable or considered surgically incurable. Singe-agent cisplatin is recommeded as the chemotherapeutic agent of choice in concurrent chemotherapy. The routine use of adjuvant chemotherapy following either surgery or radiotherapy is not recommended. Multidisciplinary tumour board discussions are beneficial in making decisions about precise treatment protocols.
The Role of Surgery in Head and Neck Cancer Treatment
Surgical resection is the primary treatment for stage I-II oral cancer. Pending the pathological results of clear margins, extracapsular extension in metastatic lymph nodes or lymphovascular invasion, post-operative radiation may be considered. Often, post-op radiation is contemplated as a planned combined approach. Again multidisciplinary tumour boards are the standard of care for making these difficult treatment decisions for complex cases.
A surgical procedure, mandibulotomy involves splitting the mandible to gain access to the floor of mouth and tongue.


This is an example of a 78F patient who was treated surgically with a mandibulotomy procedure, partial glossectomy and post-operative radiation therapy for a squamous cell carcinoma of the tongue. It can be seen that the patient was unable to lift the tongue secondary to the surgery to optimize the panoramic radiograph emphasizing the airway shadow over the roots of the maxillary anterior teeth. Reapproximation of the sectioned mandibular segments by fixation with 2 titanium plates is evident. Complications that may arise include: loss of vitality and mobility of the teeth adjacent to the resection line, malocclusion and temporomandibular joint pain.
Mandibulotomy procedures and the the use of reconstruction techniques utilizing free vasularized grafts provide opportunities for the dentist to be part of the team to restore function. Apart from the logistical difficulties, participation of maxillofacial prosthodontists in the surgical planning (e.g fabrication of surgical splints) is important in the rehabilitation and restoration of function and aesthetics. When radiation therapy is not part of the cancer therapy, implant retained prostheses are possible and can aid in rehabilitation.

In this example, resection (mandibulectomy) post-chemotherapy for an osteosarcoma of the left mandible has left a defect that was restored with a partial lower denture initially and later by osseous integrated implants as radiation therapy was not delivered.
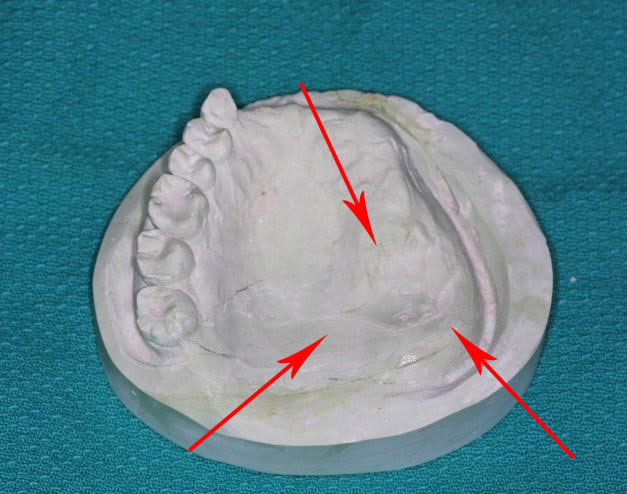
The following is an example of a surgical splint. The arrows outline the site of a mucoepidermoid carcinoma of the left maxillary turberosity and palate area in a 39 yr-old female patient who was partially edentulous in the maxilla. The first step involves making an alginate impression of the upper arch. The model is then reviewed by the head and neck surgeon who outlines the extent of the surgical resection. A clear acrylic splint was made to cover the area of the surgical site. The splint is then delivered to the operating room where the surgeon inserts it at the time of resection. It may be fixed in place with palatal screws depending on the retention. When the patient awakens in the recovery room, function is immediately established without the need for a feeding tube. The patient is also able to speak intelligibily. The surgical splint is left in place for the immediate post-operative period. As healing progresses, the margins of the resection shrink leading to leakage of the temporary obturator. Soft reline materials are used to fill the voids until healing is complete and a permanent prosthesis can be fabricated.