Metastases
Metastases to the Head and Neck
Updating the medical history of all patients at each visit is essential. Patients who have developed a malignancy since their last dental visit require a review of systems of the disease. Certain malignancies, such as breast and prostate carcinomas have a propensity to metastasize to bone and can bypass the thoracic cavity by hematogenous spread via the paravertebral Batson’s plexus of valveless veins. i.e. the patient does not need to have widespread metastases to have a lesion in the jaws or oral soft tissues.
Metastatic tumors to the oral soft tissues and jaws represent only 1-3% of all oral cancer with the most common primary sites being the lung, breast, kidney, prostate and liver. They may present with dental symptoms of pain, swelling or mobile teeth often making the dentist the initial health care provider seen. Other symptoms include paresthesia and non-healing extraction sites. The dentist is in the unique position in that radiographs of the area are usually readily attainable. Close observation of the image and careful clinical history should raise the level of suspicion to make the diagnosis of a metastatic lesion. The radiographic features of metastases are similar as for malignancy in bone. Metastatic tumors are more commonly found in the posterior mandible, but can occur anywhere in the bone or soft tissues. The periphery is ill-defined with lack of cortication. The destruction is not well-demarcated and can be described as infiltrative or moth-eaten or patchy. The irregular destruction of the normal bony trabeculae gives rise to a more radiolucent background. Widening of the periodontal ligament space and destruction of the lamina dura may also be seen. Other cortical boundaries such as the inferior border of the mandible, the sinus floor and posterior border of the maxilla may also be involved. Rarely tooth roots are resorbed resulting in conical shaped roots.
Case Examples:
Case 1:
66M with a history of gastric carcinoma with liver metastases presented to the dentist complaining of pain and swelling in the upper right.




Observations & Discussion:
There are obvious sources of dental infection in the first quadrant. Deep buccal caries of tooth 15, a carious root of #14 and retained root tips of #16. The buccal swelling obliterating the buccal vestibule adjacent to #15 appears more fleshy than fluctuant and extends mesially with a sharper border than would be expected with strictly inflammatory disease. Of note in the periapical film is loss of the lamina dura part way down the distal portion of the root of #15 with irregular bone destruction. These features are indicative of a metastatic lesion rather than a dental inflammatory one. Incisional biopsy of the swelling revealed a solid soft tissue mass which on histologic examination was consistent with metastases from gastric carcinoma.
Case 2:
58M with known lung cancer presented to his dentist with an irregular mass emanating from the buccal attached gingiva of tooth #23.




Observations & Discussion:
An irregular nodular mass that was ulcerated is present on the attached gingiva of the upper left cuspid. It extends to cover the cervical portion of the crown of the tooth. There are several smaller yellowish papules on the surface in the superior aspect. A periapical radiograph was exposed. Given the clinical appearance and radiographic features, the differential diagnosis included pyogenic granuloma, periodontal abscess or fibrous epulis. With the history of lung cancer, the possibility of a metastatic lesion from the lung was also considered. An incisional biopsy revealed this to be a squamous cell carcinoma consistent with lung primary. In this case, the radiograph did not show characteristics of malignancy.
Case 3:
67F had completed radiation therapy for an adenoid cystic carcinoma of the paranasal sinuses with extension into the middle cranial fossa. There were known metastases in the liver and lung. She presented 6 months later with a painful nodular swelling on the right lateral tongue. On biopsy, it was confirmed to be another metastatic focus. Because of the multiple metastases after recent radiation therapy, she was referred for palliative care.


Case 4:
This 67 yr-old female had an autologous stem cell transplant for multiple myeloma 1.5 years previously. She had been on intravenous bisphosphonates since that time and presented to her dentist with a painless swelling distal to tooth #27.




Observations & Discussion:
The fleshy mass posterior to the upper left second molar is the same colour as the surrounding mucosa. It appears firm and not inflammatory in nature. The periapical film of the area shows an ill-defined area of bone destruction in the left tuberosity with remnants of remaining trabeculae. There is some widening of the periodontal ligament space on the distal of 27 with loss of the alveolar bone. Of note as well, the lamina dura around the roots of the 25,26 and 27 is thickened. It is particularly prominent along the entire distal root surface of the 25. This is in keeping with the history of intravenous bisphosphonate therapy. The soft tissue was biopsied and the pathology report confirmed a plasma cell lesion consistent with multiple myeloma. Because of this, chemotherapy was initiated and the mass reduced considerably in size.
Case 5:
This 56 year-old woman presented with pain and limited opening. She had known metastatic breast cancer.




Observations & Discussion:
There is an ill-defined radiolucent entity in the superior portion of the right mandibular ramus. There is some sclerosis at the periphery. Unfortunately, there is overlap of the airway over the region of interest. This lesion does not require biopsy for diagnosis. An MRI ordered by her oncologist would be sufficient to make the diagnosis. Often these painful areas are treated with local radiation therapy as a palliative measure.
Case 6:
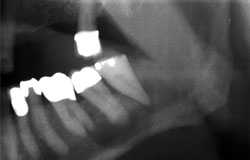
This 48 year-old female presented with pain and paresthesia of the left mandible. She had been treated for lung cancer.


Observations & Discussion:
The quality of this film is suboptimal. However, multiple infiltrative destructive radiolucencies can be seen in the left body of the mandible extending to the lower cortex which is no longer uniform in density compared to the right side. The radiographic features are highly suggestive of malignancy and if there is no soft tissue swelling, an MRI would confirm the diagnosis without biopsy.
Case 7:
This 62 yr-old man presented with a painful swelling of the posterior mandibular gingiva. It had gradually increased in size over the past 2 months. He had a history of kidney cancer.






Observations & Discussion:
There is an obvious ulcerated fleshy mass in the buccal vestibule of the third quadrant. It is lobulated and appears firm. It extends from the first bicuspid region to the retromolar pad and covers some of the posterior teeth. The radiograph revealed an ill-defined radiolucent entity surrounding the roots of the lower left third molar #38. There is loss of the lamina dura with no appreciable peripheral bone reaction. The soft tissue mass can be seen in the cropped pantomograph.
Case 8:
This 61 year-old female presented with pain and difficulty opening her mouth. She had been treated for thyroid cancer in 2 years previously.


Observations & Discussion:
This cropped pantomograph of the right mandible shows a destructive lytic lesion of the condyle. The recent onset of her pain and trismus most likely coincided with pathologic fracture of the condyle.
Case 9:
This 64 year-old man with known metastatic prostate cancer was referred to the dental clinic to rule out a dental abscess vs. metastatic oral lesion.






Observations & Discussion:
There is poor oral hygiene and obvious poor dentition. A large erythematous mass is present emanating from the buccal attached gingiva of the upper right second molar (#17). The mass extends to cover the buccal surface of the crown of the tooth. The tooth was mobile and sensitive to percussion. The periapical film shows a change in trabecular pattern of bone posterior to the molar from destruction of the bone. However, the superior extent cannot be appreciated. A soft tissue mass correlates with the clinical appearance. There is loss of the lamina dura which may be mistaken as periapical or periodontal inflammatory disease. The cropped pantomograph shows loss of the posterior border of the maxilla and an irregularly widened periodontal ligament space around the mesial surface 17. This underscores the importance of imaging the entire lesion.
Case 10:
This 79 year-old man complained of bleeding from his mouth at night. He had known mandibular metastasis of his lung cancer.





Observations & Discussion:
The pantomorgraph reveals advanced bone destruction of the rami bilaterally without expansion or much effect on surrounding structures. This results in “tooth floating in space” appearance.
Case 11:
This 46 yr-old female had known history of metastatic breast cancer and presented to her dentist with swelling in the anterior mandibular region. There was some mild tenderness to touch and occasional tingling.



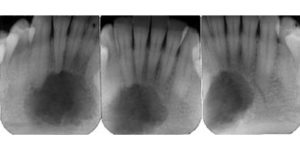
Observations & Discussion:
The films reveal a central radioucent area with ragged edges and little peripheral bone reaction. The tangential extraoral occlusal film shows destruction of the buccal plate of the mandible. Although not characteristic of breast carcinoma metastases, a biopsy revealed that it was an adenocarcinoma consistent with breast cancer.
The above examples show the protean nature of metastases to the jaws and oral soft tissues. Appropriate imaging to encompass the entire lesion is essential to delineate the borders and careful review of the clinical findings given a prior history of cancer are all important to make this critical diagnosis. The radiographic changes are often subtle and clinical appearance may resemble dental disease. Given that the incidence of metastases to the oral hard and soft tissues is rare, clinical experience and careful review of the history should raise a level of suspicion in the astute diagnostician. Referral of the images to an oral and maxillofacial radiologist, if available is recommended.