Osteoradionecrosis
Osteoradionecrosis (ORN) is a serious complication that occurs in irradiated bone where there is damage to all of the components of bone. In our current database, there are 330 patients diagnosed with ORN indicating an approximate incidence of 2.5%. This is likely under reported because this is often a late effect occurring many years after treatment. Therefore, many patients are either lost to follow-up or are seen at other centres years following radiation treatment. From this large number, our experience has given some insight into the nature of this process.
Radiation damage to bone may be seen as a spectrum dependent primarily on the dose to the bone itself with other mitigating patient factors such as comorbidities such as continued tobacco use, poor dental care/oral hygiene and overall health of the patient. Traditionally, ORN has been described by Marx as bone exposure from a sequence of radiation induced hypoxic, hypocellular, hypovascular tissue which break downs often secondary to trauma leading to a chronic non healing wound. Infection was not seen as a primary etiology. More recently, it has been proposed that the radiation induces fibrosis and atrophy, damage to endothelium with inflammation and vascular thrombosis resulting in tissue necrosis.
Radiation damage has been described extragnathically in the long bones, femoral head and neck, pelvis and ribs. In these sites, the presentation is that of fracture. In the jaws, discussion here is centred on the mandible as it is far more frequently involved than the maxilla. Possible reasons for this include the fact that the dose received by the mandible in head and neck radiation is greater than the maxilla (due to the proximity of metastatic lymph nodes), the anatomic structure of the mandible and the presence of teeth. The mandible is unique in that it is a membranous bone with a central vascular supply consisting predominantly of the inferior alveolar nerve (V-III) with a high cortical/trabecular ratio of bone. The rest of the vascular supply to the jaw is predominantly through the periosteum. With thin mucosal covering in the sites where ORN occurs most frequently (the lingual retromolar/mylohyoid region), minor trauma may expose bone that has a reduced capacity to heal.
It has been our experience that there is a spectrum of change to the bone that responds to the injury of radiation and that this may change with time. It is often a late effect and may occur years after the radiation treatment. This is an important factor in patient education – that the risk is lifelong so that he/she must strive to maintain a healthy dentition and prevent extractions. Cone beam CT has been very useful in determining the number, size and location of sequestra. The accessibility of sequestra for removal with minimal invasive surgery is important to ascertain prior to treatment.
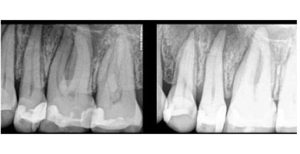
The response of bone to the trauma of radiation is inflammation. This is seen radiographically as an increase in sclerosis. Sclerosis in bone makes the bone denser – more trabeculae and less vascular. Healing requires remodeling. Irradiated bone has less ability to remodel. There are limits to the tolerance of injury and trauma that bone can withstand. Radiation therapy (as well as other insults such as bisphosphonate therapy) can be considered as macrotrauma that lower the threshold of the ability for bone to repair. Adding in microtrauma events such as dental extraction, denture irritation, break in mucosal protection from traumatic ulceration may lead to exceeding the bone’s capacity to remodel resulting in necrosis and sequestra formation. When the sequestrum is superficial, bone exposure may occur. The signs and symptoms usually prompt the patient to present for care. When the sequestrum is deeper within the bone or inaccessible to the oral cavity, radiographic signs may be the only diagnostic features. Radiographic features of radiation damage to the jaws without bone exposure include widening of the periodontal ligament space, sclerosis and sequestra formation. Because of research done in our clinic, (King Chong Chan, Susanne E. Perschbacher, et al : Mandibular changes on panoramic imaging after head and neck radiotherapy, Oral Surg Oral Med Oral Pathol Oral Radiol 2016;121:666-672)) these changes have been recognized as important features for dentists to be aware to prevent unnecessary treatment which may predispose to ORN. Thorough radiographic examination is important to delineate these changes. Long term follow-up imaging has been useful in detecting changes.
Example 1
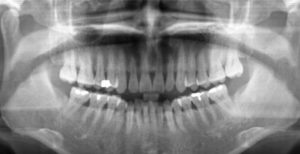
This 66F underwent 70Gy of radiation in 2009 for a right base of tongue squamous cell carcinoma.


Nov, 2009


July, 2014
Observations and Discussion:
The 2014 image reveals irregular widening of the periodontal ligament spaces of the 36 and 37. There is increased sclerosis between the 35 and 36. The teeth in the second quadrant show similar changes.
The molars in the third quadrant are totally asymptomatic. They are neither sensitive to percussion or mobile. It is important to recognize that these changes are secondary to the radiation therapy and NOT to odontogenic causes. Extraction or root canal therapy is not only contraindicated but carry significant risk of the development of ORN.
Example 2
This 59M was treated in 2012 for base of tongue squamous cell carcinoma with chemoradiation (70 Gy in 35 fractions)


Apr, 2012


Mar, 2015
Observations and Discussion:
The patient presented as an emergency in 2015 having been lost to follow-up for 2 years. He had pain in the posterior right mandible and trismus. Tooth #48 (lower right wisdom tooth) was tender to percussion. He was treated with antibiotics. The radiograph revealed irregular periodontal ligament space widening. Periapical rarefying osteitis would be centred around the apices of the tooth and periodontal bone loss would be originating at the alveolar crest. This radiographic change was interpreted as being secondary to radiation therapy. His symptoms certainly indicated infection; however, the infection may have involved the tooth secondarily. He was treated with antibiotics alone and has been asymptomatic for over a year. Extraction would carry the risk of the development of ORN and should be avoided if possible.
Example 3
This 48F was treated for right base of tongue squamous cell carcinoma in 2004. She was taking oral bisphosphonates for osteoporosis.

Aug, 2004


July, 2009


Oct, 2014
Observations and Discussion:
The initial pre-treatment pantomograph showed mild generalized periodontal bone loss. The upper left third molar was removed prior to treatment. She developed pain in the right mandible in 2009 and saw her general dentist who extracted the 45 and 46. She developed ORN of the right mandible subsequent to the extractions. There is obvious widening of the periodontal ligament space of the lower posterior teeth bilaterally. The 2014 pantomograph shows the bone destruction in the right mandible, however the appearance of the molars on the left side do not appear to have the same appearance as 5 years earlier. It may be that the widened PDL is a reversible change.
ORN Definition/Criteria
There have been many definitions and staging systems for ORN. It has been our experience that the traditional Marx definition of bone exposure without healing for 6 months does not take into consideration size of the exposure; if more than one site is affected, radiographic changes and lesions where the bone is not exposed to visual examination but is exposed to the oral cavity through fistulas. Therefore, we have created the following definition that is meaningful for our purposes:
- Bone exposure greater than one month’s duration greater than 1 cm in size and less than 2 cm;
- Bone exposure greater than one month’s duration with two or more contiguous sites, each measuring greater than 5 mm and less than 1cm
- Bone exposure greater than 3 months duration between 5 mm and 1 cm in size with radiographic evidence of radiation damage to bone including: bone resorption, bone sclerosis, widening of the periodontal ligament space and periodontal disease-like bone loss;
- No bone exposure but oral/skin fistula and radiographic evidence of sequestra formation and/or inflammatory periosteal bone formation;
- No soft tissue changes but obvious radiographic evidence of sequestra formation and/or inflammatory periosteal bone formation
- Pathologic fracture with radiographic changes consistent with radiation damage or sequestra formation with or without periosteal bone formation;
Clinical Stage 1
- Bone exposure greater than one month’s duration greater than 1 cm in size and less than 2 cm;
- Bone exposure greater than one month’s duration with two or more contiguous sites, each measuring greater than 5 mm and less than 1cm
- Bone exposure greater than 3 months duration between 5 mm and 1 cm in size with radiographic evidence of radiation damage to bone including: bone resorption, bone sclerosis, widening of the periodontal ligament space and periodontal disease-like bone loss;
Clinical Stage 2
- Bone exposure greater than one month’s duration greater than 2 cm in size and less than 4 cm;
- Bone exposure greater than one month’s duration with two or more contiguous sites, each measuring greater than 1 mm and less than 3cm
- Bone exposure greater than 3 months duration >2 cm in size with radiographic evidence of radiation damage to bone including: bone resorption, bone sclerosis, widening of the periodontal ligament space and periodontal disease-like bone loss;
- No bone exposure but oral/skin fistula and radiographic evidence of sequestra formation and/or inflammatory periosteal bone formation;
- No soft tissue changes but obvious radiographic evidence of sequestra formation and/or inflammatory periosteal bone formation
Clinical stage 3
- Pathologic fracture with radiographic changes consistent with radiation damage or sequestra formation with or without periosteal bone formation;
Clinical features of ORN:
The most common anatomic site for bone exposure post therapeutic radiation is the posterior mandible in the retromylohyoid lingual region. This is most likely due to a number of factors. First of all, this area often receives a higher dose of radiation because of the proximity of level 1 lymph nodes which often require treatment. Also, the mucosa covering the mandible is this region is thinner and more likely to become traumatized easily.
This is an example of a very superficial area of bone exposure in the lingual portion of the alveolar ridge in the edentulous 36 site. The small shell of bone can be easily removed without local anaesthetic to leave intact mucosa. This does not represent ORN but it illustrates the type of “sequestrectomy” that can be performed as part of conservative therapy.




Clinical examples:
1
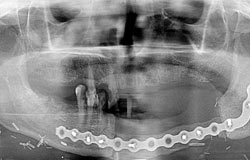
This 60M was treated for a left hypopharyngeal squamous cell carcinoma in Dec, 2012. He had very large mandibular tori and a 35 pack/year history of smoking. He presented in Feb, 2015 with exposed bone on the posterior right lingual torus.




This pantomograph was exposed in Aug 2015. There is an abnormal bone pattern of both sides of the mandible. The left side showed irregular areas of bone sclerosis and bone resorption with the presence of several sequestra extending from the height of the alveolar process to include the inferior cortex of the mandible. The findings on the right side are less prominent and involve the alveolar processof the mandible extending from the retromolar region to the first molar area. These findings are consistent with osteoradionecrosis on both sides.


He underwent hyperbaric oxygen therapy (30 dives) then proceeded to have the right sided tori surgically removed. This pan was exposed Jul, 2016 and shows more extensive involvement on the left side


2
This 80F was treated for a squamous cell carcinoma of the left maxillary alveolus in 2008. She received 70Gy of radiation and 2 cycles of chemotherapy. There was a recurrence eighteen months later and she had surgery. She presented with bone exposure of the left mandible in 2014. She returned monthly for sequestrectomy and had no further bone exposure 1 year later. She had a 50 pack/year history of smoking.


3
This 54F was treated for a squamous cell carcinoma of the left mandibular alveolus in 2014 with chemotherapy and radiation after surgical resection with reconstruction. She had a 30 pack/year history of smoking. She presented 7 months later with bone exposed mesial to tooth #43. There is post-radiation caries of the remaining teeth but no radiographic evidence to indicate ORN in this case; however, the bone exposure is sufficient for the diagnosis of ORN.



4
This 61F was treated for a squamous cell carcinoma of the posterior right retromolar trigone and received 60 Gy in 25 fractions 10 years prior to this photograph and image. She has a 50 pack/year history of smoking. There are 2 separate areas of bone exposure in the right mandibular alveolar ridge. This occurred after her general dentist extracted tooth #44 one year earlier. The appearance of the body of the right mandible is abnormal and consistent with ORN. This example underscores that the risk of ORN is lifelong and extractions are contraindicated for life.



5
This 57F was treated with 66 Gy post-operatively for an adenoid cystic carcinoma of the left palate in December, 2012. She presented in June, 2014 with this area of bone exposure and change in the periapical radiograph indicative of radiation damage. She was treated with hyperbaric oxygen and periodic sequestrectomy as pieces of bone became loose in the site. There was complete mucosal coverage by January, 2016. ORN is more commonly seen in the mandible with some precipitating factor such as tooth extraction. This example illustrates spontaneous ORN in the maxilla.



6
63M treated for a right oropharyngeal carcinoma with radiation. After his treatment he had a lower partial denture made and presented with bone exposure from the new denture. This example emphasizes the need for patients, even if edentulous to seek treatment for denture sores post-radiation.


7
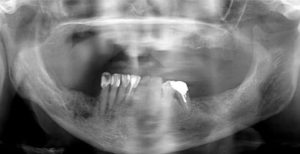
This 66F refused surgical resection of a right sided tongue squamous cell carcinoma in May of 2002 and received radiation only. She presented in May, 2004 stating that a tooth fell out and this photograph was taken. She refused treatment as she stated that she was not having any pain and could still eat. She had a 50 pk/yr history of smoking.


May, 2002


May, 2004


This radiograph reveals extensive post-radiation caries and widened periodontal ligament spaces of the mandibular teeth.
She returned in Dec 2004 with a more extensive area of bone exposure and spontaneous exfoliation of tooth #44




This film was exposed in Mar, 2005. The radiographic report included: There are numerous areas of increased radiolucency in the mandible extending from the second bicuspid area on the left side to the first molar area on the right side. A portion of the inferior mandibular cortex is eroded in the right anterior area. No periosteal response is present. The periodontal ligament spaces of the remaining mandibular teeth are widened. These changes are consistent with the previous diagnosis of osteoradionecrosis affecting the mandible.



This film was exposed Feb, 2006. The osteoradionecrosis extends from approximately the third molar region on the right side of the mandible to the first molar region on the left side. The difference between this film in the previous film is that the degree of bone involvement is greater with profound involvement of the inferior cortex. There is the risk of a pathologic fracture. This final film was taken in July 2007 after a pathologic fracture necessitated removal of the necrotic mandible with bone grafting.
8
68M firefighter received 70Gy of radiation with concurrent chemotherapy for a T3N1 squamous cell carcinoma of the left retromolar trigone and tonsil in 2003. He was placed on an oral bisphosphonate in 2005 for osteoporosis having undergone bilateral knee replacements. He had tooth #18 (upper right third molar) extracted in Jan 2006 and tooth #46 removed Feb, 2006. In 2008, he presented with areas of bone exposure – right and left posterior maxilla and posterior right mandible. Interestingly, the radiographs taken did not reveal any evidence of sequestra, sclerosis or widening of the periodontal ligament spaces. We believe that this is an example of osteonecrosis associated with oral bisphosphonates complicated by radiation therapy and extractions. It may be that bone has a certain tolerance in its ability to heal. Radiation therapy, bisphosphonate use and trauma may be additive insults that lower this threshold.






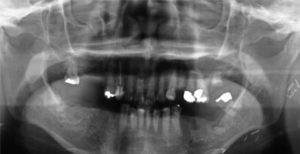
9
60F with right base of tongue carcinoma received chemoradiation in 2004. In 2010, teeth 45 and 46 were very mobile and there was a purulent exudate emanating from the gingival crevices of both teeth. The panoramic film shows evidence of radiation damage with widened periodontal ligament spaces of the lower molars. Teeth 45 and 46 were extracted in 2 separate appointments in late 2010 and early 2011. The healing was very slow and she returned monthly for sequestrectomies. Clnically, the sockets can be clearly seen with bone at the base exposed. The radiographic report in 2014 indicated an abnormal bone pattern involving the body of the right mandible extending from approximately the cuspid region to the base of the mandibular ramus. Within this region are irregular areas of bone sclerosis and the bone resorption. There does appear to be several small sequestra and is consistent with osteoradionecrosis. Interestingly, the widened PDL space of the left mandibular molars does not appear as prominent as in 2009.

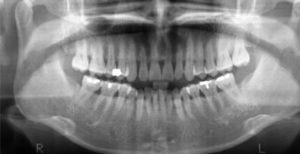
2004


2009


2014


10
This 74M was treated in 2003 with radical radiation therapy for an unknown primary with metastases to the left neck. He was well until he returned in 2011 with swelling in the left mandible and bone exposed around the remaining molar (#37). It was otherwise asymptomatic and not mobile or sensitive to percussion. This was treated conservatively with chlorhexidine rinses and sequestrectomies as pieces of bone became loose. He had a 50 pk/yr history of smoking and was finally able to quit in Feb 2012. He developed purulent exudate from the site and was treated with hyperbaric oxygen (HBO) in planning for extraction of the tooth. It was extracted after 6 weeks of HBO in Sept, 2012. He had slow healing with sequestra being removed monthly for 4 months. He developed a pathologic fracture in December, 2012. This required a partial mandibulectomy with a scapular vascularized graft.


2003


2011


2012


2013
11
This 60F was treated twice for nasopharyngeal carcinoma, first at the age of 38 in 1991 and secondly for supraclavicular nodal metastases in 2003. She did not use her Fluoride trays and had extensive post-radiation caries. All of her remaining teeth were extracted in 2007 and complete dentures were made for her. She presented in May, 2012 with paresthesia of the lower left lip and on examination had thick pus draining from a small fistula in the left posterior mandibular alveolar ridge. The radiographic report indicated an abnormal bone pattern involving the body of the left mandible. This is composed of irregular regions of sclerosis and bone resorption with several sequestra. These changes are consistent with osteoradionecrosis. A pathologic fractured occurred 4 months later. Resection of the left mandible was carried out but reconstruction was not possible.

2004

May, 2012


Aug, 2012


Oct, 2013
12
This 65F was treated in 1992 for a squamous cell carcinoma of the right tonsil with XRT. She had a 20 pk/yr history of smoking and ethanol abuse. In 2007, she developed pain and infection in the right mandible and it was removed after several courses of antibiotics did not effect any improvement. A diagnosis of ORN was made and she was successful in smoking cessation. She continued to have intermittent flare-ups of pain, infection with purulence and in 2009 after hyperbaric oxygen therapy had surgical removal of tooth #48 and sequestrectomy. She has been symptom free since that time.


Feb, 2007


Apr, 2009


Oct, 2011
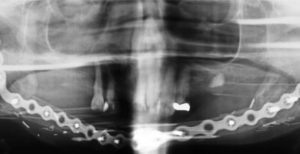
13
This 59M was treated for a left tonsil squamous cell carcinoma in 2003 with external beam radiation of 70 Gy. He presented 10 years later in 2013 complaining of pus draining from the wisdom tooth on the lower left. A sinugram was performed and a region of bone destruction inferior to the IAN can be seen. This would correspond to a high dose site. There was no bone exposed. A cone beam CT showed multiple areas of cortical destruction. He underwent HBO and sequestrectomy via an extraoral approach and was asymptomatic until 2015 when tooth #38 required extraction because of infection. Shortly after the extraction, he developed a pathologic fracture. He has had a partial mandibulectomy with scapular graft reconstruction.


Apr, 2013






14
80F with a T3N0 squamous cell carcinoma of the left retromolar trigone and floor of mouth treated with 60 Gy in 25 fractions radiation therapy in 2009. Her medical history was significant for oral bisphosphonate therapy for osteoporosis and had a 30-40 pk/yr history of smoking. In 2013, her dentist extracted tooth #36 and she developed osteoradionecrosis and a pathologic fracture. Of note are the compounding factors of smoking and oral bisphosphonate use.


2009


2013


2014
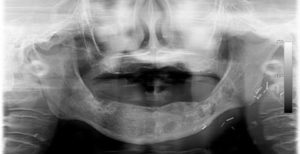
15
This 85M was treated for an T3N0 nasopharyngeal carcinoma in 1992 at the age of 61. He had a tooth extracted in the posterior left mandible in 2013. Since that time he has had repeated episodes of swelling and pain in the area and presents with an opening of the skin with purulent drainage. There was no exposed bone intraorally. Of note is that he was taking an oral bisphosphonate, Fosamax up until 2015. Because of his age, he declined surgical resection and was treated with hyperbaric oxygen alone. The pantomograph exposed in 2015 reveals a destructive lesion in the posterior left mandible with pathologic fracture. The pantomograph from 2016 shows a continuous lower border of mandible although sequestra are still present.


2015


2016
16
This 74F was treated in 2006 for a nasopharyngeal carcinoma with concurrent chemotherapy and radiation. She was being treated for osteoporosis with Actonel and hypertension with Norvasc. Her dentist extracted the lower right molar in 2009 after which she sustained a pathologic fracture. She was treated with hyperbaric oxygen and antibiotics and healed without surgery.

2009


2010
17
This 59M treated for NPC 2008 – with radiation alone. Sequence of 6 pantomographs reveal changes culminating in pathologic fracture of the right mandible after teeth have become progressively loose and symptomatic requiring extraction.


2010


2012


2013

2015


2016


2017
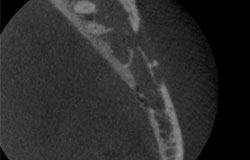
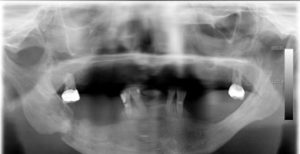
18
This 81F with adenoid cystic carcinoma of the left submandibular gland treated with surgery and post-operative radiation therapy in 2012. At that time the lower left first molar was not mobile or symptomatic, so a decision was made to leave it in place so as not to delay her radiation. In 2013 she developed severe pain associated with the 36 and it was extracted. It appeared to heal uneventfully. In August 2014, she presented with bone exposure at the site and in 2015 sustained a pathological fracture.


2012


Apr, 2015


Oct, 2015

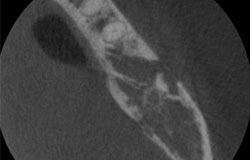


The cbCt coronal axial slice shows loss of the buccal cortex in the 36 area with a subjacent sequestrum. There is piecemeal destruction of the lingual cortical plate. This may be better appreciated on the coronal view as endosteal scalloping of the lingual cortical plate. The superior portion buccal cortical plate in this view appears separated from the mandible and is a sequestrum. The density in the centre may be representative of the dense bone island which is also a sequestrum.
Treatment
The treatment of osteoradionecrosis is variable depending on the severity (stage) and clinical symptoms. It may range from simple sequestrectomy, irrigation and antibiotics as needed to hyperbaric oxygen therapy with surgical debridement of sequestra to resection. Maintenance of the lower border of the mandible is a goal of therapy. Clinical trials using a regimen of pentoxifylline, Vitamin E, clodronate and steroids shows some promise in improving healing and may be useful before extraction in the radiated jaw. The use of collagen plugs, primary closure and antibiotic coverage may also improve healing when extractions are necessary. Currently, patient education to prevent extractions by using the topical home fluoride and maintaining good dental health are paramount in achieving this. However, when extractions are inevitable, leaving a smaller wound to heal by not taking out adjacent teeth at the same appointment may be beneficial. For example, if a patient returns that requires multiple extractions post-radiation due to dental neglect, it may be optimal to extract one tooth per quadrant per month to allow for healing before proceeding to adjacent teeth.
Summary from our experience
- Osteoradionecrosis is a highly morbid condition of necrosis of bone that has been exposed to therapeutic radiation. Its incidence is not decreasing with IMRT radiation and the addition of chemotherapy. Treatment is unpredictable in stage 2. For stage 1, conservative treatment consisting of superficial sequestrectomies and chlorhexidine rinses/irrigation can often lead to healing. Surgical resection of the involved jaw may be necessary for stages 2 and 3.
- The most common precipitating event is dental extraction.
- First determine if the tooth actually requires extraction and that the radiographic evidence of widening of the periodontal ligament is not the only reason for this determination. Signs and symptoms of infection may not necessarily be related to the teeth. It may be necessary to treat with antibiotics to make this determination
- Continued smoking and oral bisphosphonate use increase the risk of ORN development with post –XRT extractions.
- Radiographic evaluation with pantomographs on a regular (1-2 years) basis is helpful in following up on high risk patients.
- Cone beam CT is beneficial in delineating the number and location of sequestra