Chemotherapy
Chemotherapy is a general term referring to cancer treatment that is drug or medication based. i.e. not radiation or surgery. Historically, it was first introduced in the 1940’s when mustard gas used in World War I was found to cause lower blood counts in exposed individuals. Because of this, it was thought that it may be of use in cancer and was initially used for lymphoma. Today there are many different types of chemotherapy agents that work in many different ways. Some of them will predispose the patient to bleeding or infection and routine dental care may not be safe.
Chemotherapy drugs are numerous and vastly different in their effects on tumors and normal tissues. Traditionally, chemotherapeutic agents are cytotoxic to cells that are rapidly dividing. This is aimed at the cancer cells, but many other normal cells that are turning over rapidly may also be affected. These may result in mucositis and pancytopenia. These agents have the potential to be myelosuppressive and this carries significance for safe dental care. These agents are often used in combination and are given in cycles that have been determined by clinical trials. Other types of chemotherapy include anti-hormone receptor agents, immunotherapy and targeted agents. The hormone receptor agents are primarily used as an adjunct in breast and prostate cancers that are promoted by hormones.
For the most part, myelosuppression is the major concern affecting safe dental care. Thrombocytopenia and neutropenia may preclude invasive dental treatment as excessive bleeding and infection may result. Knowing the agents, dosage regimen and the blood counts are important in determining whether safe care can be administered. Consultation with the medical oncologist will provide information regarding the timing of care. After myelosuppressive chemotherapy, the blood counts will drop and expose the patient to risks of bleeding and infection. Depending on the agent used, the blood counts will gradually recover before the next cycle of chemotherapy is to be administered. Generally, elective dental care is not advisable during chemotherapy that is myelosuppressive. Timing of emergency dental care is very important. Elective dental care is not recommended. Recovery of the blood counts to acceptable levels usually occurs before the next dose or cycle of chemotherapy. It is at this time that emergency dental care can be provided. Neutropenia (PMN <1) may require the use of prophylactic antibiotics. Thrombocytopenia presents challenges for dental extractions. Other emergency care such as endodontic therapy, placing sedative dressings, smoothing of rough or fractured surfaces and denture adjustments may be performed if administration of local anaesthetics can be safely done. For example, mandibular block anaesthesia should be avoided in the patient with low platelets because of the risk of vascular events. Consultation with the oncologist and knowledge of the current blood work are necessary for safe dental care.
Chemotherapy Treatment Strategies
Chemotherapy is often combined with other treatment modalities such as radiation therapy or surgery. Combined modality strategies include: neoadjuvant, when the agent is given prior to local treatment such as surgery to shrink the primary tumor first; Concurrent – where the chemotherapy agents are given at the same time as another type of therapy such as radiation; Adjuvant – where it is given after local treatment to lower the risk of recurrence and metastases.
- Induction chemotherapy is the first line of treatment of cancer with curative intent.
- Consolidation chemotherapy is given after remission in order to prolong overall disease-free time and improve overall survival. The same agent is used that achieved remission by induction.
- Intensification chemotherapy is the same as consolidation but a different agent is used than the first one that achieved remission.
- Maintenance chemotherapy refers to repeated low dose treatment to prolong remission.
- Palliative chemotherapy is used to reduce tumor load to increase life expectancy and reduce symptoms
Chemotherapy Types
- Myelosuppressive
- Hormone receptor agents
- Immunotherapy
- Targeted agents
Myelosuppressive means depression of the bone marrow. Erythroid and myeloid precursors may be affected leading to pancytopenia which may result in anemia, leukopenia, and thrombocytopenia. In general, the mechanism of action of these agents is relatively non-specific in that they target all cells that are rapidly dividing with the intent of being cytotoxic to cancer cells. This class is the most common type used and may render your patient unfit for elective dental care as the risk of bleeding and infection may be significant. Emergency care necessitates knowing the current blood counts especially the platelet and neutrophil count.
Myelosuppressive agents work in many different ways. Some are cytotoxic to cells during mitosis by preventing spindle formation or disassembly; others prevent DNA synthesis while others work by arresting the cell cycle. Myelsuppressive agents fall into the following categories:
- Alkylating agents
- Anthracyclines
- Antimicrotubular
- Antimetabolites
Alkylating agents attach an “alkyl” group to DNA. This alkyl group attaches to a guanine base of the purine ring. This prevents the DNA from replicating because the cross linkages formed prevent uncoiling of the DNA double helix. These agents would affect all cells that divide rapidly such as the mucosal lining of the gut, oral cavity, bone marrow and gonads. Examples of alkylating agents include: cyclophosphamide, procarbazine, dacarbazine, melphalan, chlorambucil and busulfan. Carboplatin and cisplatin are platinum based and do not contain an alkyl group but work in a similar fashion by crosslinking DNA strands. They are considered to be alkylating-like agents. They are used in head and neck cancer, multiple myeloma, leukemia and lymphoma.
Anthracyclines are a class of antibiotic drugs derived from Streptomyces bacterium. They inhibit DNA and RNA synthesis. They work by inserting molecules between the 2 strands of DNA; generating highly reactive free radicals that damage other molecules; and by inhibiting topoisomerase I and II. These enzymes work to to allow normal unwinding of DNA during replication and transcription. Inhibiting them causes breaks in the DNA. Examples include daunorubicin and doxorubicin (Adriamycin®) which are used in combination with other agents for Hodgkin’s disease, leukemia, breast, stomach, uterine ovarian, bladder and lung cancers.
Antimicrotubular agents inhibit disassembly of the mitotic spindle and cause breakage of chromosomes. They bind to microtubules stabilizing them so that they do not dissemble. This leads to a significant decrease in free tubulin which is needed for microtubule formation. This results in inhibition of mitosis. The microtubules accumulate within the cell and cause the initiation of apoptosis (cell death). Examples include docetaxel (Taxotere®). Paclitaxel (Taxol®, Abraxane®). They are used in metastatic breast cancer, metastatic prostate cancer, lung cancer and advanced head and neck cancer. Vinca alkaloids, derived from the periwinkle plant bind to tubulin protein stopping the cell from separating chromosomes during metaphase. Examples include vincristine and vinblastine which are used in lymphoma, leukemia and lung cancer.
Antimetabolite agents are a group of drugs that impede DNA and RNA synthesis. They have similar structures to nucleotide base purines (guanine and adenine) and pyramidines (cytosine, thymine and uracil).They become incorporated into DNA or block DNA polymerase required for DNA synthesis thereby preventing mitosis. Examples include methotrexate, fludarabine, fluorouracil, gemcitabine, cytarabine, hydroxyurea and azacitidine. They are widely used in many different types of cancer but especially in metastatic breast cancer and leukemia.
Myelosuppressive agents are often combined into “cocktails”. The combination of different agents allows for lower doses of each thereby decreasing the toxicity and chances of resistance to any one particular agent. They do increase the effect of myelosuppression. They are commonly given acronym nicknames that may include trade names for ease of nomenclature. There are many different types of cocktails that are used and pending results of clinical trials, they are constantly changing. Common examples follow:
- CHOP (used in non-Hodgkin’s lymphoma)
- Cyclophosphamide
- Hydroxydaunorubicin
- Oncovin® (Vincristine)
- Prednisone
- R-CHOP (used in non-Hodgkin’s lymphoma)
- Same as above with the addition of Rituximab
- VAD (used in multiple myeloma)
- Vincristine
- Adriamycin® (Doxorubicin)
- Dexamethasone
- ABVD (Used in Hodgkin’s disease)
- Adriamycin® (Doxorubicin)
- Bleomycin
- Vinblastine
- Dacarbazine
- MOPP (used in Hodgkin’s disease)
- Mechlorethamine (nitrogen mustard)
- Oncovin® (Vincristine)
- Prednisone
As part of the cocktail, steroids are often included as either prednisone or dexamethasone. They act as immunosuppressants in myeloproliferative diseases and also work to decrease some of the side effects of the cytotoxic agents.
These agents are delivered in cycles. This refers to dosing regimens based on protocols for each disease and stage. The cycles allow for a recovery period between doses. The timing and doses are evidence based determined by clinical trials. Different myelosuppressive agents vary in their effect on the bone marrow, the maximal depression of the bone marrow is referred to as the “nadir’ and may take a few days after the initial dose to occur depending on the agent used. The nadir refers to the point in time when the blood counts are the lowest. It is at this time that thrombocytopenia, neutropenia, and anemia can predisposed to bleeding, infection and sepsis. This is the most undesirable time for any dental care. The blood counts usually recover after this point, but depending on the agents used and the patients overall health, the time that this takes is variable. Consultation with the oncologist is necessary to determine if safe dental care can be provided. It is important in the functional enquiry to learn the date of the last chemotherapy cycle and when the next one is scheduled. This gives some indication of the recovery time but knowing the blood counts is essential. In general, the best time to perform emergency dental care only is immediately prior to the next cycle of chemotherapy when the counts have recovered enough for another dose. This is predicated on the blood counts.
Normal Blood Counts
| Males | Females | |
|---|---|---|
| Hemoglobin (Hb) | 140-180g/L | Females 120-160 g/L |
| White Blood cell count (WBC) | 4.0-11.0 x 10 -9/L | |
| Platelets | 150-450 x 10-9/L | |
| Neutrophil count (PMN) | 2.0-7.5 x 10-9/L | |
Systemic Side effects
Not all myelosuppressive agents will cause all of these effects. Most non-specific agents will cause hair loss, but many of the other effects are dependent of the type of agent used. For example, anthracyclines are known to cause cariotoxicity. Some of these effects are temporary such as hair loss, fatigue ad GI upset; others such as infertility and secondary malignancies are not.
As of June 30, 2015 the Head and neck cancer patients seen in our clinic by site was 12,727 with the following breakdown:
- Hair Loss
- Anemia, fatigue
- GI upset – dysguesia, anorexia, nausea, vomiting, constipation and diarrhea
- Peripheral neuropathy
- Otoxicity – hearing loss
- Cognitive impairment
- Infertility
- Risk of secondary malignancies
- Organ damage – hart, liver, kidney
- Skin – dry skin, damaged nails
Oral effects of myelosuppression
Mucositis, neutropenic ulceration, dysgeusia, opportunistic infections (eg. Candidiasis, HSV), xerostomia, tooth sensitivity are potential oral complications of myelosuppressive chemotherapy.
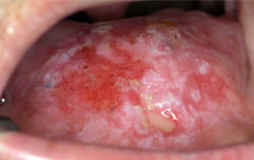


Mucositis with erythema and ulceration occurs because the oral mucosal epithelial cells turn over rapidly and as such are targeted by some of the myelosuppressive agents. This causes pain and difficulty with nutrition.




The photograph on the left side is of a painful ulcer in the buccal mucosa of a patient undergoing induction chemotherapy for leukemia. The neutrophil count was below 0.5. The photograph on the right is of the same patient 2 weeks later when the neutrophil count had increased to 1.7. Neutropenic ulcers characteristically are coated with a film of bacteria.






Opportunistic infections secondary to neutropenia may also occur with myelosuppression. Candidiasis and herpes simplex are the most common infections in the immunosuppressed patient.
Treatment of Oral Side Effects
Relief of discomfort is the objective in the treatment of the oral side effects. They are self limiting and usually resolve when the blood counts return to acceptable levels. Mouthrinses such as simple baking soda and water, topical anesthetics such as lidocaine viscous, topical antifungal agents are the mainstay of empiric treatment. Patients may also obtain some symptomatic relief by sucking on ice chips. As these side effects are temporary, keeping the patient comfortable so that maintenance of nutrition is possible is the goal of therapy.
Hormone antineoplastics
Hormone antineoplastics are used in tumors which thrive on hormones. The most common include breast and prostate carcinomas. This form of therapy is usually given as maintenance after other primary modalities. As they are aimed at reducing levels of hormones, myelosuppression is not a complication and these drugs do not affect the ability to provide safe invasive dental care.
Examples include Letrozole (Femara®) and Tamoxifen. The former is an aromatase inhibitor which converts androgens to estrogen leading to a decrease in circulating estrogen. It is generally used in post-menopausal women as adjuvant treatment for breast cancer. Tamoxifen competitively binds with estrogen receptors on tumor cells decreasing the estrogen effects, and preventing division of the tumor cells.
In prostate cancer, antiandrogens block and inhibit testosterone which acts to promote growth of certain prostate cancers. Examples include Degarelix (Firmagon®) and Abiraterone (Zytiga®). The former blocks GNnRH (gonadotropin releasing hormone) in the anterior pituitary gland by reversibly binding to the receptor. This results in a decrease in LH (lutenizing hormone) and FSH (follicle stimulating hormone) causing a drop in testosterone levels. The latter works by inhibiting the enzyme needed for androgen synthesis in prostate tumor tissue and inhibits the formation of testosterone precursors.
Immunotherapy
Immunotherapy in the context of chemotherapy refers to boosting the normally functioning immune system to attack the tumor cells. There are myriad mechanisms possible given the complex nature of the immune response. This is a burgeoning area of research. Examples include:
- Interferons. These are cytokines produced by white blood cell. Many of their functions include activation of natural killer cells and macrophages, increasing host defenses. Interferon alpha 2b (Intron®) interferes with oncogene expression, inhibits cell groth and augmetns lymphocyte cytotoxicity. It has been used in malignant melanoma and kaposi’s sarcoma.
- Alemtuzumab (MabCampath®) – this enhances antibody dependent cell mediated cytotoxicity. It has been used in B-CLL and is now used in multiple sclerosis
- Nivolumab – allows the immune system to attack the tumor by blocking PD-L1 (programmed death ligand). It has been used in melanoma and non small cell lung carcinoma
- Ipilimumab (Yervoy®) – is a monoclonal antibody that activates the immune system by targeting a protein receptor that allows cytotoxic t lymophocytes to recognize and destroy cancer cells. It is used in melanoma.
- Rituximab (Rituxan®) – targets the CD 20 receptor on B lymphocytes activating antibody and complement mediated cytotoxicity. It is used in lymphoma and leukemia.
- Thalidomide – is antiangiogenic and suppresses excess tumor necrosis factor and increases NK cells. It is used in multiple myeloma.
- Lenalidomide (Revlimid®) – is a potent inhibitor of TNF∂ and inhibits growth of myeloma cells by inducing cell cycle arrest and cell death. It is used as maintenance chemotherapy in multiple myeloma.
Targeted Chemotherapy
Targeted agents are monoclonal antibodies to specific genes or gene products of the abnormal cancer cell. Because they ‘target’ the cancer cells or their products specifically, there are less systemic side effects. They are often used in combination with other agents. Some examples include:
- Imatinib (Gleevec®) – is a tyrosine kinase inhibitor. Tyrosine kinase is an enzyme of the mutant gene that occurs with chronic myelogenous leukemia
- Bortezomib (Velcade®) – a proteasome inhibitor. Proteasomes are protein complexes inside cells that regulate degradation of unneeded or damaged proteins. It is used in multiple myeloma and mantle cell lymphoma
- Cetuximab (Erbitux®) – is an epidermal growth factor receptor (EGFR) inhibitor. Some epithelial cancer cells have receptors on their surfaces that bind to a normal protein called epidermal growth factor (EGF). This activates the cell to divide and grow. The receptor inhibitor will bind to the receptor so that EGF and its activity is blocked. It is used in colon and head and neck squamous cell cancers.
- Blinatumomab (Blincyto®) – is a targeted immunotherapy agent. It is a bi specific T cell engager. It links the T cell to malgnant B cell so that the T cell kills the malignant B cell. It is used in refractory acute lymphoblastic leukemia.
- Bevacizumab (Avastin®) – binds vascular endothelial growth factor (VEGF) resulting in blocking the formation of new blood vessels needed for tumor growth. It is used in metastatic colon cancer.
- Trastuzumab (Herceptin®) – binds to the Human Epidermal Growth Factor Receptor (HER2) preventing the binding of human epidermal growth factor which stimulates cell proliferation. In approximately 25% of breast cancers the HER2 is overexpressed causing the cancer cells to reproduce uncontrollably. It is used in breast cancer that shows this overexpression of the HER2 or those that are HER2-positive.
Clinical Trials
Patients may present to the dental office and reveal in their medical history that they are on a clinical trial or a study for treatment of their cancer. This information may impact on safe dental care and it is necessary to contact the oncologist or study nurse to get information. Frequently, this infers that the disease is refractory to the usual therapy and may be palliative in nature. If the patient is a part of a randomized controlled trial (RCT) comparing differing treatments, communication with the oncologist or study nurse is necessary.
Pre-Chemotherapy Dental Objectives
- Remove potential sources of odontogenic infections – this may require extractions or root canal therapy
- Create a healthy oral enviroment
Pre-Chemotherapy Dental Protocol
- Thorough medical history
- Clinical examination
- Radiographic examination
- Remove and treat potential sources of odontogenic infection
- Restoration of large carious lesions – may require sedative dressings
Summary
If there is a sufficient window of opportunity to remove areas of infection and potential areas of infection, undertake a cleaning, scaling and oral hygiene instruction this should be done. The dental examination should be a complete, thorough examination and include a complete radiographic examination. The keystone of treatment is infection removal.
To better prepare you for patients requiring chemotherapy treatment ask them to bring a copy of their complete blood count, any coagulation laboratory tests and a complete list of their chemotherapy drugs including the doses and the timing of treatment. You can find information on the many chemotherapy regimens online or in a drug reference text. Patients should also discuss the timing of dental treatment with their oncologist who ideally should give the go-ahead. There are a few critical issues in the management of patients on some chemotherapy regimens that cause immunosuppression.
Be mindful that most patients with central venous catheters may require antibiotic coverage to prevent the catheter from becoming infected.
Always treat the patient in your comfort zone from a hematological standpoint – i.e. factor in their hemoglobin level, their platelet count, any coagulation disturbances and their absolute neutrophil count. Everyone’s comfort zone is different and it differs from patient to patient and procedure to procedure. Generally during chemotherapy treatment it is better to err on the side of caution. The best way of preventing complications of treatment is to not cause them.